

CABG Versus PCI: Greater Benefit in Long-Term Outcomes With Multiple Arterial Bypass Grafting
- PMID: 26403338
- PMCID: PMC5473156
- DOI: 10.1016/j.jacc.2015.07.060
CABG Versus PCI: Greater Benefit in Long-Term Outcomes With Multiple Arterial Bypass Grafting
Abstract
Background: Treatment of multivessel coronary artery disease with traditional single-arterial coronary artery bypass graft (SA-CABG) has been associated with superior intermediate-term survival and reintervention compared with percutaneous coronary intervention (PCI) using either bare-metal stents (BMS) or drug-eluting stents (DES).
Objectives: This study sought to investigate longer-term outcomes including the potential added advantage of multiarterial coronary artery bypass graft (MA-CABG).
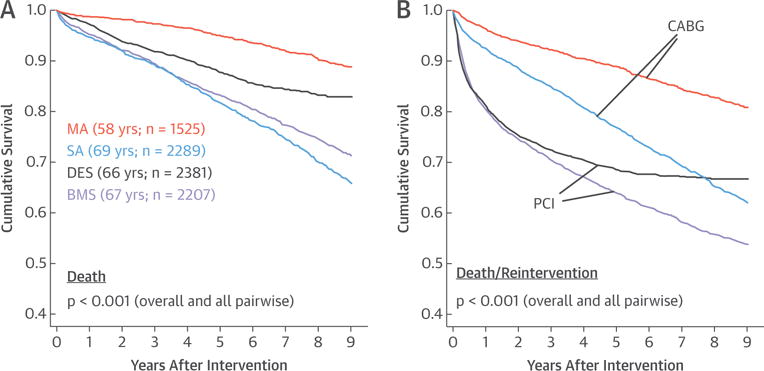
Methods: We studied 8,402 single-institution, primary revascularization, multivessel coronary artery disease patients: 2,207 BMS-PCI (age 66.6 ± 11.9 years); 2,381 DES-PCI (age 65.9 ± 11.7 years); 2,289 SA-CABG (age 69.3 ± 9.0 years); and 1,525 MA-CABG (age 58.3 ± 8.7 years). Patients with myocardial infarction within 24 h, shock, or left main stents were excluded. Kaplan-Meier analysis and Cox regression were used to separately compare 9-year all-cause mortality and unplanned reintervention for BMS-PCI and DES-PCI to respective propensity-matched SA-CABG and MA-CABG cohorts.
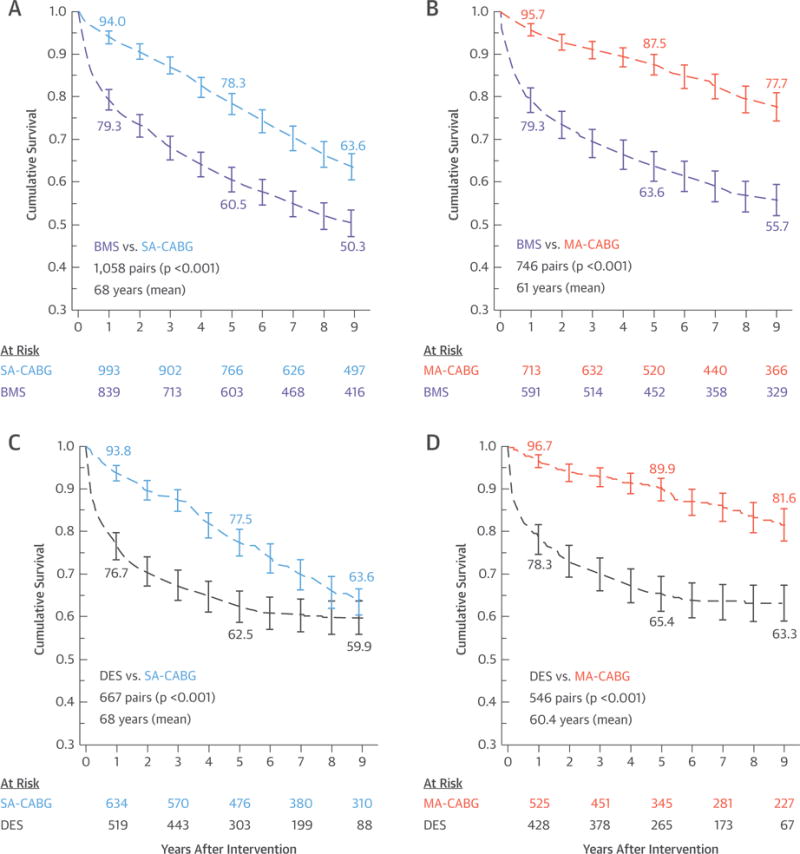
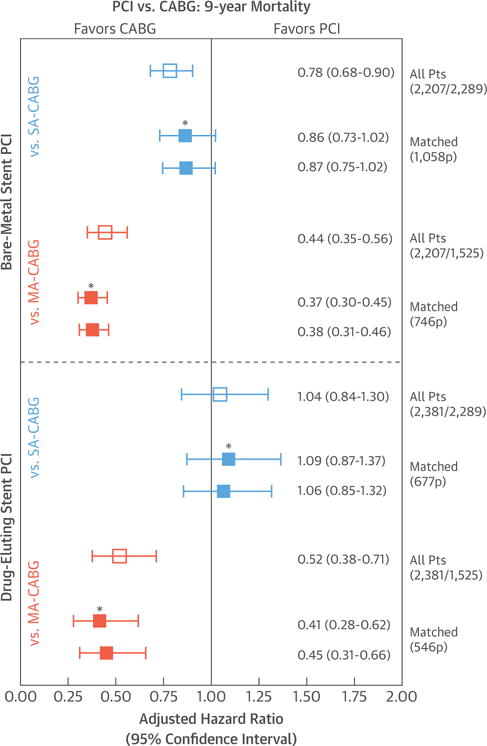
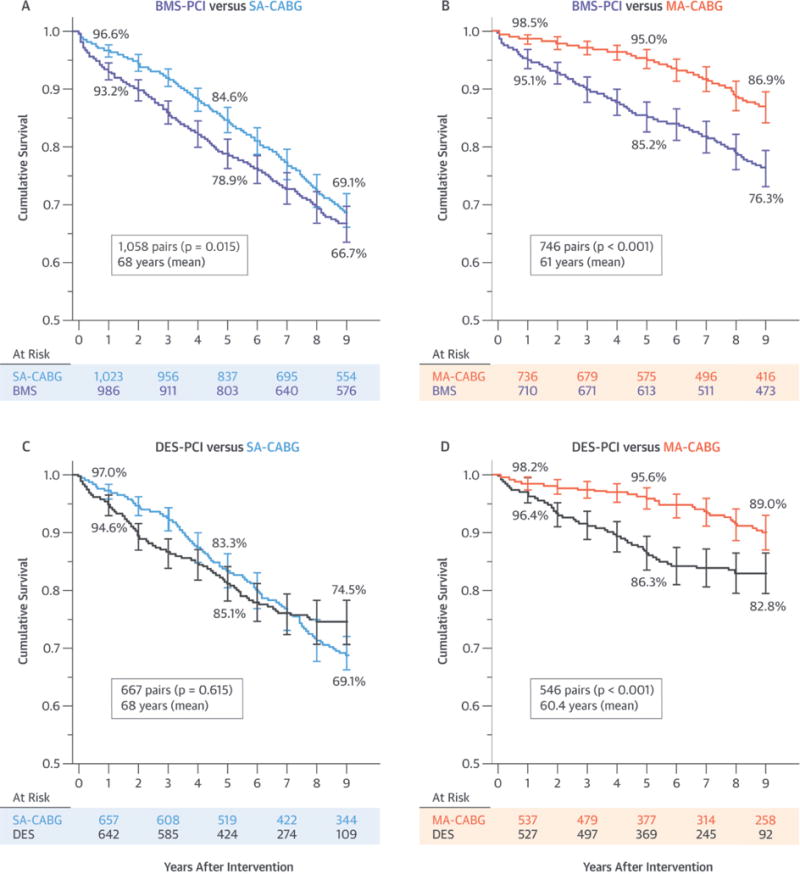
Results: BMS-PCI was associated with worse survival than SA-CABG, especially from 0 to 7 years (p = 0.015) and to a greater extent than MA-CABG was (9-year follow-up: 76.3% vs. 86.9%; p < 0.001). The surgery-to-BMS-PCI hazard ratios (HR) were as follows: versus SA-CABG, HR: 0.87; and versus MA-CABG, HR: 0.38. DES-PCI showed similar survival to SA-CABG except for a modest 0 to 3 years surgery advantage (HR: 1.06; p = 0.615). Compared with MA-CABG, DES-PCI exhibited worse survival at 5 (86.3% vs. 95.6%) and 9 (82.8% vs. 89.8%) years (HR: 0.45; p <0.001). Reintervention was substantially worse with PCI for all comparisons (all p <0.001).
Conclusions: Multiarterial surgical revascularization, compared with either BMS-PCI or DES-PCI, resulted in substantially enhanced death and reintervention-free survival. Accordingly, MA-CABG represents the optimal therapy for multivessel coronary artery disease and should be enthusiastically adopted by multidisciplinary heart teams as the best evidence-based therapy.
Keywords: arterial grafting; coronary stents; myocardial revascularization; propensity matching.
Copyright © 2015 American College of Cardiology Foundation. Published by Elsevier Inc. All rights reserved.
Conflict of interest statement
The authors have reported that they have no relationships relevant to the contents of this paper to disclose. Richard Shemin, MD, served as Guest Editor for this paper.
Figures
Comment in
-
Multiple Arterial Coronary Bypass Grafting: Likely Better, But Not Yet a Mandate.J Am Coll Cardiol. 2015 Sep 29;66(13):1428-30. doi: 10.1016/j.jacc.2015.08.012. Epub 2015 Aug 13. J Am Coll Cardiol. 2015. PMID: 26279097 No abstract available.
-
CABG Versus PCI: Are All Revascularization Strategies Created Equal?J Am Coll Cardiol. 2016 Mar 29;67(12):1503-1504. doi: 10.1016/j.jacc.2015.11.070. J Am Coll Cardiol. 2016. PMID: 27012415 No abstract available.
-
Reply: CABG Versus PCI: Are All Revascularization Strategies Created Equal?J Am Coll Cardiol. 2016 Mar 29;67(12):1504-1505. doi: 10.1016/j.jacc.2016.01.026. J Am Coll Cardiol. 2016. PMID: 27012416 No abstract available.
References
-
- Serruys PW, Ong AT, van Herwerden LA, et al. Five-year outcomes after coronary stenting versus bypass surgery for the treatment of multivessel disease: the final analysis of the Arterial Revascularization Therapies Study (ARTS) randomized trial. J Am Coll Cardiol. 2005;46:575–81. - PubMed
-
- Hueb W, Lopes NH, Gersh BJ, et al. Five-year follow-up of the Medicine, Angioplasty, or Surgery Study (MASS II): a randomized controlled clinical trial of 3 therapeutic strategies for multivessel coronary artery disease. Circulation. 2007;115:1082–9. - PubMed
-
- Booth J, Clayton T, Pepper J, et al. for the SoS Investigators Randomized, controlled trial of coronary artery bypass surgery versus percutaneous coronary intervention in patients with multivessel coronary artery disease: six-year follow-up from the Stent or Surgery Trial (SoS) Circulation. 2008;118:381–8. - PubMed
-
- Kapur A, Hall RJ, Malik IS, et al. Randomized comparison of percutaneous coronary intervention with coronary artery bypass grafting in diabetic patients: 1-year results of the CARDia (Coronary Artery Revascularization in Diabetes) trial. J Am Coll Cardiol. 2010;55:432–40. - PubMed
-
- Kappetein AP, Feldman TE, Mack MJ, et al. Comparison of coronary bypass surgery with drug-eluting stenting for the treatment of left main and/or three-vessel disease: 3-year follow-up of the SYNTAX trial. Eur Heart J. 2011;32:2125–34. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
