

(68)Ga-PSMA-11 PET/CT: a new technique with high potential for the radiotherapeutic management of prostate cancer patients
- PMID: 26404016
- PMCID: PMC4771815
- DOI: 10.1007/s00259-015-3188-1
(68)Ga-PSMA-11 PET/CT: a new technique with high potential for the radiotherapeutic management of prostate cancer patients
Abstract
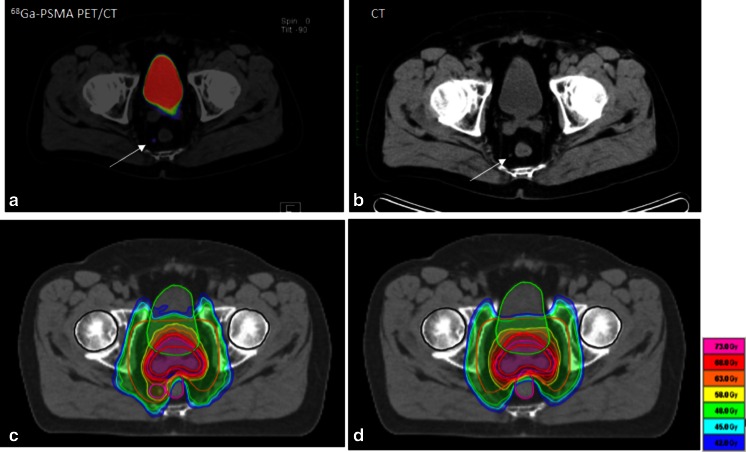
Purpose: Radiotherapy is the main therapeutic approach besides surgery of localized prostate cancer. It relies on risk stratification and exact staging. This report analyses the potential of [(68)Ga]Glu-urea-Lys(Ahx)-HBED-CC ((68)Ga-PSMA-11), a new positron emission tomography (PET) tracer targeting prostate-specific membrane antigen (PSMA) for prostate cancer staging and individualized radiotherapy planning.
Methods: A cohort of 57 patients with prostate cancer scanned with (68)Ga-PSMA-11 PET/CT for radiotherapy planning was retrospectively reviewed; 15 patients were at initial diagnosis and 42 patients at time of biochemical recurrence. Staging results of conventional imaging, including bone scintigraphy, CT or MRI, were compared with (68)Ga-PSMA ligand PET/CT results and the influence on radiotherapeutic management was quantified.
Results: (68)Ga-PSMA ligand PET/CT had a dramatic impact on radiotherapy application in the presented cohort. In 50.8 % of the cases therapy was changed.
Conclusion: The presented imaging technique of (68)Ga-PSMA PET/CT could be a key technology for individualized radiotherapy management in prostate cancer.
Keywords: 68Ga-PSMA ligand PET/CT; Individualized radiotherapy; Prostate cancer; Radiotherapy planning.
Figures



References
-
- Kuru TH, Roethke MC, Seidenader J, Simpfendörfer T, Boxler S, Alammar K, et al. Critical evaluation of magnetic resonance imaging targeted, transrectal ultrasound guided transperineal fusion biopsy for detection of prostate cancer. J Urol. 2013;190(4):1380–1386. doi: 10.1016/j.juro.2013.04.043. - DOI - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
