

Stent-Assisted Coil Embolization of Intracranial Aneurysms: Complications in Acutely Ruptured versus Unruptured Aneurysms
- PMID: 26405089
- PMCID: PMC7960113
- DOI: 10.3174/ajnr.A4542
Stent-Assisted Coil Embolization of Intracranial Aneurysms: Complications in Acutely Ruptured versus Unruptured Aneurysms
Abstract
Background and purpose: The use of stents in the setting of SAH is controversial because of concerns about the efficacy and risk of dual antiplatelet therapy. We compare complications of stent-assisted coil embolization in patients with acutely ruptured aneurysms with complications in patients with unruptured aneurysms.
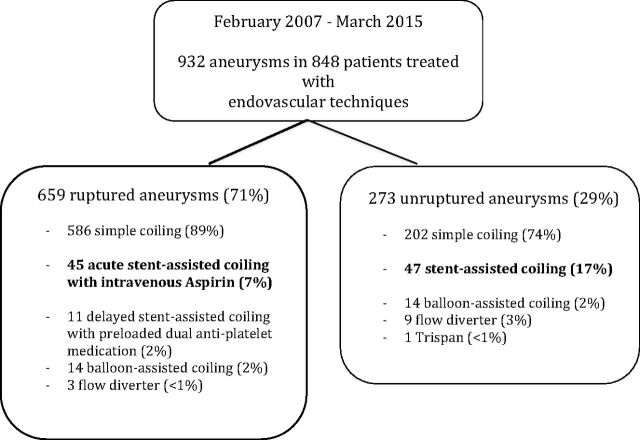
Materials and methods: Between February 2007 and March 2015, 45 acutely ruptured aneurysms and 47 unruptured aneurysms were treated with stent-assisted coiling. Patients with ruptured aneurysms were not pretreated with antiplatelet medication but received intravenous aspirin during the procedure. Thromboembolic events and early rebleeds were recorded.
Results: In ruptured aneurysms, 9 of 45 patients had thromboembolic complications. Four patients remained asymptomatic, 4 developed infarctions, and 1 patient died. The permanent complication rate in ruptured aneurysms was 11% (95% CI, 4%-24%). Five of 45 patients (11%; 95% CI, 4%-24%) had an early rebleed from the treated aneurysm after 3-45 days, and in 4, this rebleed was fatal. In 46 patients with 47 unruptured aneurysms, thromboembolic complications occurred in 2. One patient remained asymptomatic; the other had a thalamus infarction. The complication rate in unruptured aneurysms was 2.2% (1 of 46; 95% CI, 0.01%-12%). No first-time hemorrhages occurred in 46 patients with 47 aneurysms during 6 months of follow-up.
Conclusions: The complication rate of stent-assisted coiling with early adverse events in ruptured aneurysms was 10 times higher than that in unruptured aneurysms. Early rebleed accounted for most mortality. In ruptured aneurysms, stent-assisted coil embolization is associated with increased morbidity and mortality and should only be considered when less risky options have been excluded.
© 2016 by American Journal of Neuroradiology.
Figures
References
MeSH terms
LinkOut - more resources
Full Text Sources
Medical