

doi: 10.1093/cid/civ720.
Epub 2015 Sep 24.
Patterns of Hydrocephalus Caused by Congenital Toxoplasma gondii Infection Associate With Parasite Genetics
Affiliations
- PMID: 26405147
- PMCID: PMC4657535
- DOI: 10.1093/cid/civ720
Item in Clipboard
Patterns of Hydrocephalus Caused by Congenital Toxoplasma gondii Infection Associate With Parasite Genetics
Clin Infect Dis.
.
Abstract
Four anatomical patterns of hydrocephalus secondary to congenital Toxoplasma gondii infection were identified and characterized for infants enrolled in the National Collaborative Chicago-based Congenital Toxoplasmosis Study. Analysis of parasite serotype revealed that different anatomical patterns associate with Type-II vs Not-Exclusively Type-II strains (NE-II) (P = .035).
Keywords: Toxoplasma gondii; aqueductal obstruction; foraminal obstruction; hydrocephalus.
© The Author 2015. Published by Oxford University Press on behalf of the Infectious Diseases Society of America. All rights reserved. For Permissions, please e-mail: journals.permissions@oup.com.
Figures
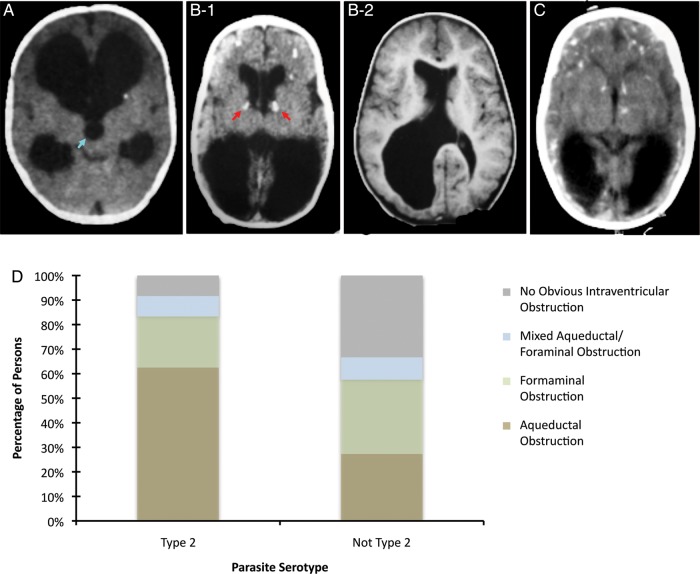
Anatomical patterns of hydrocephalus in congenital Toxoplasma gondii infection and association with parasite strain. The large dark areas in the neuroimages indicate the dilated ventricular regions and hydrocephalus. A, Obstruction of the aqueduct of Sylvius; aqueduct of Sylvius indicated by blue arrow. B1, Bilateral obstruction of the foramina of Monro; foramina of Monro indicated by red arrow. B2, Unilateral obstruction of the foramina of Monro. C, No obvious intraventricular obstruction causing ventricular dilatation. D, Twenty-four patients had antibodies to Type-II peptides, and 33 had antibodies to NE-II peptides. Type-II strains were associated with aqueductal obstruction and NE-II strains were associated with nonobstructive hydrocephalus (P = .035). % Total = (Number of patients with antibodies to parasite strain and pattern of hydrocephalus/Total number of patients with antibodies to parasite strain) × 100.
Comment in
-
Effect of Antenatal Treatment on the Severity of Congenital Toxoplasmosis.Clin Infect Dis. 2016 Mar 15;62(6):811-2. doi: 10.1093/cid/civ1035. Epub 2015 Dec 21. Clin Infect Dis. 2016. PMID: 26689954 No abstract available.
-
Reply to Wallon and Peyron.Clin Infect Dis. 2016 Mar 15;62(6):812-4. doi: 10.1093/cid/civ1036. Epub 2015 Dec 21. Clin Infect Dis. 2016. PMID: 26689955 Free PMC article. No abstract available.
References
-
- Koppe JG, Loewer-Sieger DH, de Roever-Bonnet H. Results of 20-year follow-up of congenital toxoplasmosis. Lancet 1986; 1:254–6. - PubMed
-
- McAuley J, Boyer KM, Patel D et al. Early and longitudinal evaluations of treated infants and children and untreated historical patients with congenital toxoplasmosis: the Chicago Collaborative Treatment Trial. Clin Infect Dis 1994; 18:38–72. - PubMed
-
- Swisher CN, Boyer KM, McLeod R. Congenital toxoplasmosis. Bodensteiner JB (ed). Sem Ped Neurol 1994; 1:4–25. - PubMed
-
- Diebler C, Dusser A, Dulac O. Congenital toxoplasmosis. Clinical and neuroradiological evaluation of the cerebral lesions. Neuroradiology 1985; 27:125–30. - PubMed
-
- McLeod R, Boyer K, Karrison T et al. Outcome of treatment for congenital toxoplasmosis, 1981–2004: the National Collaborative Chicago-Based, Congenital Toxoplasmosis Study. Clin Infect Dis 2006; 42:1383–94. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
