

Cabozantinib versus Everolimus in Advanced Renal-Cell Carcinoma
- PMID: 26406150
- PMCID: PMC5024539
- DOI: 10.1056/NEJMoa1510016
Cabozantinib versus Everolimus in Advanced Renal-Cell Carcinoma
Abstract
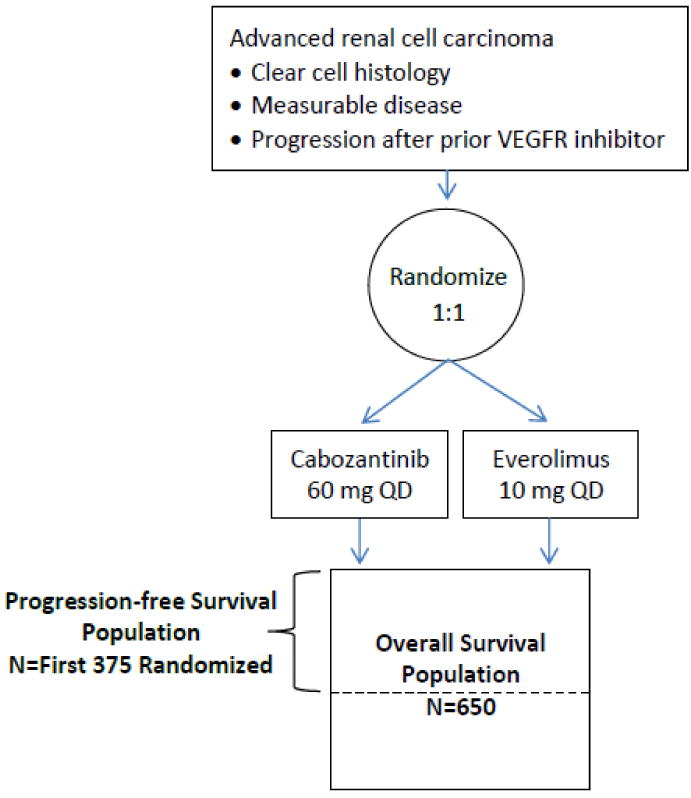
Background: Cabozantinib is an oral, small-molecule tyrosine kinase inhibitor that targets vascular endothelial growth factor receptor (VEGFR) as well as MET and AXL, each of which has been implicated in the pathobiology of metastatic renal-cell carcinoma or in the development of resistance to antiangiogenic drugs. This randomized, open-label, phase 3 trial evaluated the efficacy of cabozantinib, as compared with everolimus, in patients with renal-cell carcinoma that had progressed after VEGFR-targeted therapy.
Methods: We randomly assigned 658 patients to receive cabozantinib at a dose of 60 mg daily or everolimus at a dose of 10 mg daily. The primary end point was progression-free survival. Secondary efficacy end points were overall survival and objective response rate.
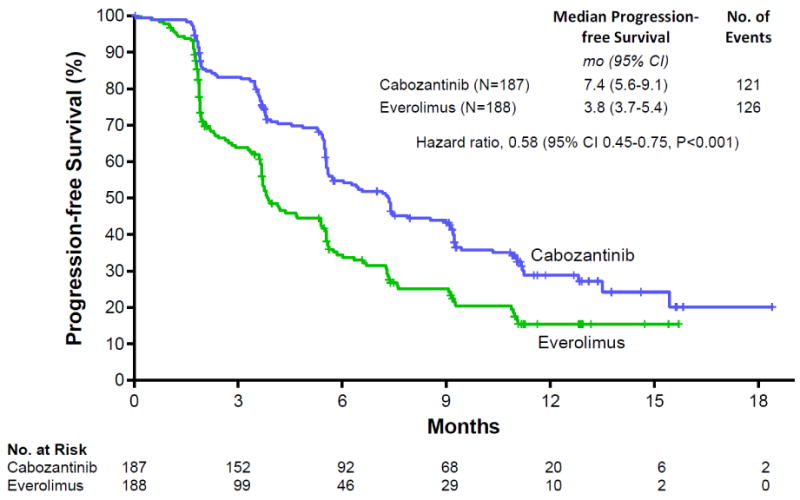
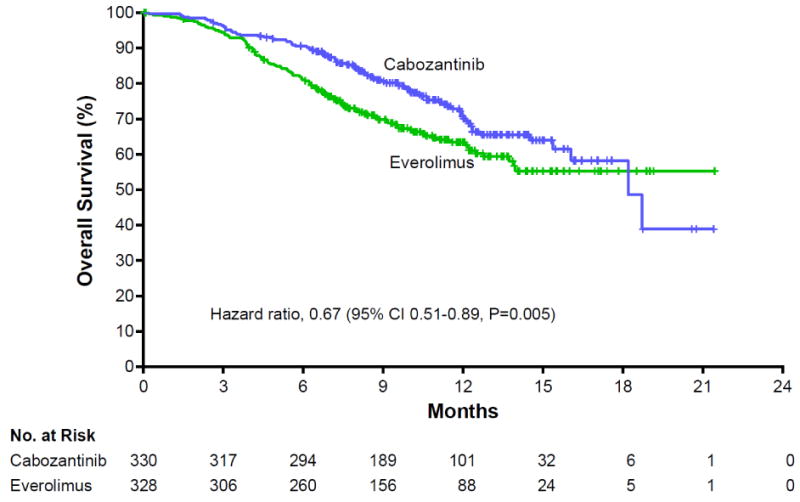
Results: Median progression-free survival was 7.4 months with cabozantinib and 3.8 months with everolimus. The rate of progression or death was 42% lower with cabozantinib than with everolimus (hazard ratio, 0.58; 95% confidence interval [CI] 0.45 to 0.75; P<0.001). The objective response rate was 21% with cabozantinib and 5% with everolimus (P<0.001). A planned interim analysis showed that overall survival was longer with cabozantinib than with everolimus (hazard ratio for death, 0.67; 95% CI, 0.51 to 0.89; P=0.005) but did not cross the significance boundary for the interim analysis. Adverse events were managed with dose reductions; doses were reduced in 60% of the patients who received cabozantinib and in 25% of those who received everolimus. Discontinuation of study treatment owing to adverse events occurred in 9% of the patients who received cabozantinib and in 10% of those who received everolimus.
Conclusions: Progression-free survival was longer with cabozantinib than with everolimus among patients with renal-cell carcinoma that had progressed after VEGFR-targeted therapy. (Funded by Exelixis; METEOR ClinicalTrials.gov number, NCT01865747.).
Figures
Comment in
-
Renal-Cell Cancer--Targeting an Immune Checkpoint or Multiple Kinases.N Engl J Med. 2015 Nov 5;373(19):1872-4. doi: 10.1056/NEJMe1511252. Epub 2015 Sep 25. N Engl J Med. 2015. PMID: 26406149 Free PMC article. No abstract available.
-
CheckMate for advanced-stage ccRCC? Nivolumab and cabozantinib aMETEORate poor survival.Nat Rev Urol. 2015 Dec;12(12):651. doi: 10.1038/nrurol.2015.246. Epub 2015 Oct 13. Nat Rev Urol. 2015. PMID: 26458750 No abstract available.
-
Kidney cancer: CheckMate for advanced-stage ccRCC? Nivolumab and cabozantinib aMETEORate poor survival.Nat Rev Clin Oncol. 2015 Nov;12(11):621. doi: 10.1038/nrclinonc.2015.178. Epub 2015 Oct 13. Nat Rev Clin Oncol. 2015. PMID: 26462125 No abstract available.
-
Words of Wisdom. Re: Nivolumab Versus Everolimus in Advanced Renal-Cell Carcinoma.Eur Urol. 2016 Apr;69(4):753-4. doi: 10.1016/j.eururo.2016.01.018. Epub 2016 Feb 18. Eur Urol. 2016. PMID: 26972496 No abstract available.
References
-
- International Agency for Research on Cancer. GLOBOCAN. Kidney Cancer estimated incidence and mortality, all ages, both sexes. 2012 http://globocan.iarc.fr/Pages/fact_sheets_population.aspx. Accessed April 2015.
-
- Gupta K, Miller JD, Li JZ, Russell MW, Charbonneau C. Epidemiologic and socioeconomic burden of metastatic renal cell carcinoma (mRCC): a literature review. Cancer Treat Rev. 2008;34:193–205. - PubMed
-
- Janzen NK, Kim HL, Figlin RA, Belldegrun AS. Surveillance after radical or partial nephrectomy for localized renal cell carcinoma and management of recurrent disease. Urol Clin North Am. 2003;30:843–52. - PubMed
-
- Kroeger N, Choueiri TK, Lee JL, et al. Survival outcome and treatment response of patients with late relapse from renal cell carcinoma in the era of targeted therapy. Eur Urol. 2014;65:1086–92. - PubMed
-
- Leibovich BC, Blute ML, Cheville JC, et al. Prediction of progression after radical nephrectomy for patients with clear cell renal cell carcinoma: a stratification tool for prospective clinical trials. Cancer. 2003;97:1663–71. - PubMed
Publication types
MeSH terms
Substances
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous