

Review
doi: 10.1016/j.cell.2015.08.068.
Preclinical mouse cancer models: a maze of opportunities and challenges
Affiliations
- PMID: 26406370
- PMCID: PMC4583714
- DOI: 10.1016/j.cell.2015.08.068
Item in Clipboard
Review
Preclinical mouse cancer models: a maze of opportunities and challenges
Cell.
.
Abstract
Significant advances have been made in developing novel therapeutics for cancer treatment, and targeted therapies have revolutionized the treatment of some cancers. Despite the promise, only about five percent of new cancer drugs are approved, and most fail due to lack of efficacy. The indication is that current preclinical methods are limited in predicting successful outcomes. Such failure exacts enormous cost, both financial and in the quality of human life. This Primer explores the current status, promise, and challenges of preclinical evaluation in advanced mouse cancer models and briefly addresses emerging models for early-stage preclinical development.
Copyright © 2015 Elsevier Inc. All rights reserved.
Figures
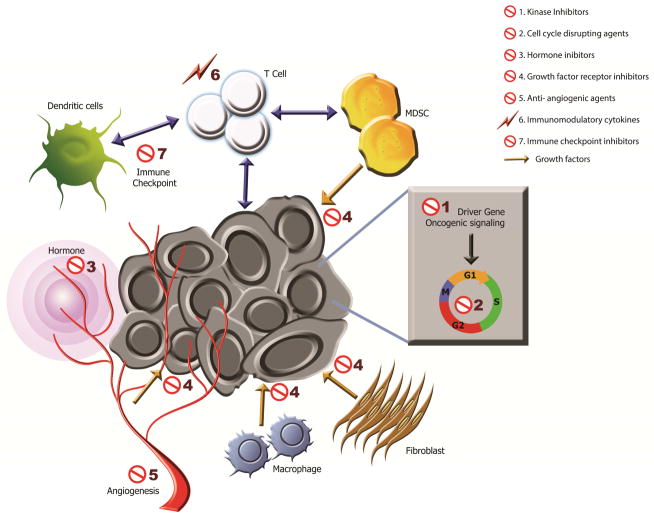
Genetic alterations produce oncogenes that drive signaling pathways in cancer cells facilitating survival and growth. However, tumor cells also cooperate with stromal cells, including vessels, fibroblasts and various immune cells, to acquire growth factors, an energy supply and protection from host defenses. These key autonomous and stromal mechanisms constitute potential therapeutic targets both locally, and for immune cells also in the circulating blood and distant immune organs. 1) Cancer cell growth driven by a mutated kinase (“Driver Gene”) can be targeted by small-molecule inhibitors. 2) Oncogenic signaling promoting uncontrolled cell cycling can be disrupted (e.g., anti-metabolites, anti-microtubule agents, DNA-damaging agents). 3 & 4) Growth of cancer cells stimulated by release of either host-derived hormones (3, concentric purple circles from blood) or growth factors (4, yellow arrows from myeloid-derived suppressor cells [MDSC], fibroblasts, macrophages, blood vessels) can be targeted by hormone inhibitors (e.g., anti-hormones or biosynthesis inhibitors) or growth factor receptor inhibitors, respectively. 5) Tumor growth requires development of new vasculature for enhanced nutrient demands, which can be blocked by anti-angiogenic agents. 6 & 7) Tumor cells can shift the inflammatory response to an immunosuppressive mode (e.g., activation of CTLA-4 and PD-1 in T cells or PD-L1 in cancer cells). The immunosuppressive environment can be reversed via treatment of immunomodulatory cytokines (6, lightning bolt; e.g., IL-2, IL-15) or immune checkpoint inhibitors (7, e.g., anti-CTLA-4, anti-PD-1, or anti-PD-L1), resuming anti-cancer activity of T cells. The cellular interactions in immune responses are marked by double-headed arrows. (Artwork by Jonathan Marie)
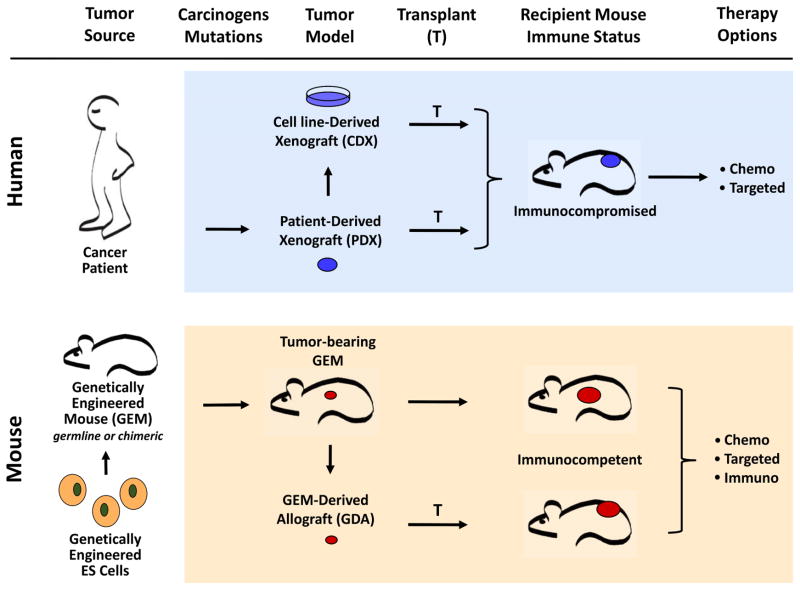
Preclinical mouse models can be defined according to the species source of tumor, how it is created, and how it is manipulated. Upper Panel) Tumors derived from human patients, and other non-murine species, can be directly transplanted into immunocompromised mice to form Patient-Derived Xenograft (PDX) models. Alternatively, these same tumors can produce established cell lines maintained in vitro as cell cultures, and transplanted into immunocompromised mice to form Cell line-Derived Xenograft (CDX) models. Since the hosts of these tumors need be immunocompromised, they are useful only for testing the efficacy of chemotherapeutics (Chemo) and targeted small-molecule inhibitors (Targeted). Xenograft models derived from canine patients also belong to this category, but are not shown here. Lower Panel) Mice can be engineered to generate tumors of human relevance with respect to histopathology, etiology and molecular wiring. Offspring of such Genetically Engineered Mice (GEM) can serve directly as preclinical models themselves, in which case the tumor is treated at its precise point of origin. Notably, model building can be streamlined by using non-germline approaches, one of which is to genetically modify ES cells and study the arising chimeric mice without time-consuming breeding schemes. Alternatively, tumors harvested from GEMs can be transplanted and expanded into fully immunocompetent syngeneic hosts, forming GEM-Derived Allograft (GDA) models. Syngeneic models allow preclinical studies of not only chemotherapeutic and small-molecule drugs, but also of all varieties of immunotherapeutic agents (Immuno).
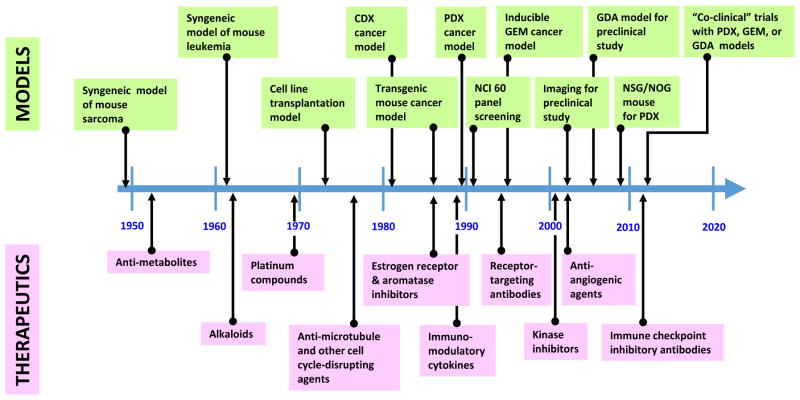
As the conceptual targets of cancer treatment progressed from actively dividing cells to oncogenic signaling and immune checkpoints, preclinical models (green boxes, upper part) and cancer therapies (pink boxes, lower part) co-evolved accordingly. This evolution was highly dependent on technical advances, resulting in waves of activity. For example, recent development of fully immunocompromised mice and diverse syngeneic GEM models has significantly promoted PDX and GDA models, respectively, for preclinical cancer studies.
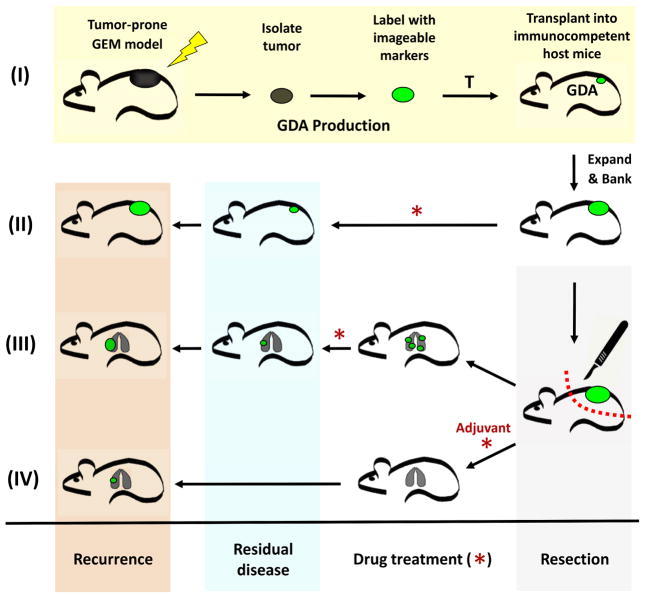
(I) GDAs are derived from tumors arising in mice genetically tailored to produce human-relevant models. Relevance can be further enhanced by including appropriate etiological agents (lighting bolt). Arising tumors are resected, labeled with imageable markers, and directly transplanted into fully immunocompetent syngeneic mice at either subcutaneously or at orthotopic. Harvested tumors can be labeled with a variety of imageable markers to monitor growth and drug response, and to FACS purify for analysis. Once successfully transplanted, GDAs can be expanded for banking and/or preclinical studies. Mice bearing GDAs can be treated directly with individual or combination drugs (*) to study therapeutic efficacy at the “primary” tumor site (II). (III and IV) Alternatively, GDAs can be resected using survival surgery, and treatments focused on metastatic disease, simulating first-line treatment in human patients following primary tumor resection. GDA models allow for interventive treatment of metastatic disease once detected (III), or preventive adjuvant treatment initiated immediately following surgical resection (IV). GDA models are thus well suiting for studying primary or metastatic disease, with interventive or preventive approaches using pathway-targeted small molecule and/or immunotherapeutic agents.
References
-
- Abate-Shen C, Politi K, Chodosh L, Olive K. Mouse Models of Cancer: A Laboratory Manual. CSHL Press; 2014.
-
- Ablain J, de The H. Retinoic acid signaling in cancer: The parable of acute promyelocytic leukemia. International journal of cancer Journal international du cancer. 2014;135:2262–2272. - PubMed
-
- Adams CP, Brantner VV. Estimating the cost of new drug development: is it really 802 million dollars? Health affairs (Project Hope) 2006;25:420–428. - PubMed
-
- Al-Lazikani B, Banerji U, Workman P. Combinatorial drug therapy for cancer in the post-genomic era. Nat Biotechnol. 2012;30:679–692. - PubMed
-
- Bailey M, Christoforidou Z, Lewis MC. The evolutionary basis for differences between the immune systems of man, mouse, pig and ruminants. Vet Immunol Immunopathol. 2013;152:13–19. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Molecular Biology Databases
