

Clinical Characteristics and Lung Function in Older Children Vertically Infected With Human Immunodeficiency Virus in Malawi
- PMID: 26407277
- PMCID: PMC5407134
- DOI: 10.1093/jpids/piv045
Clinical Characteristics and Lung Function in Older Children Vertically Infected With Human Immunodeficiency Virus in Malawi
Abstract
Background: Antiretroviral therapy (ART) has led to increased survival of children with vertically acquired human immunodeficiency virus infection. Significant morbidity arises from respiratory symptoms, but aetiology and pulmonary function abnormalities have not been systematically studied.
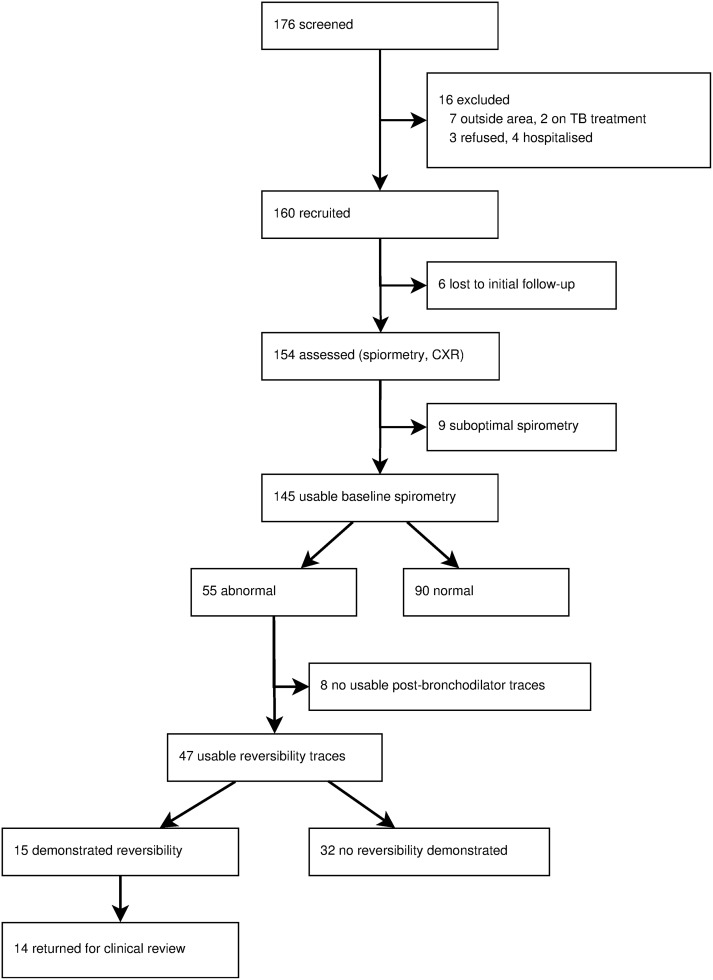
Methods: Human immunodeficiency virus-positive children aged 8-16 years were systematically recruited within clinics in Blantyre, Malawi. Clinical review, quality of life assessment, spirometry, and chest radiography were performed.
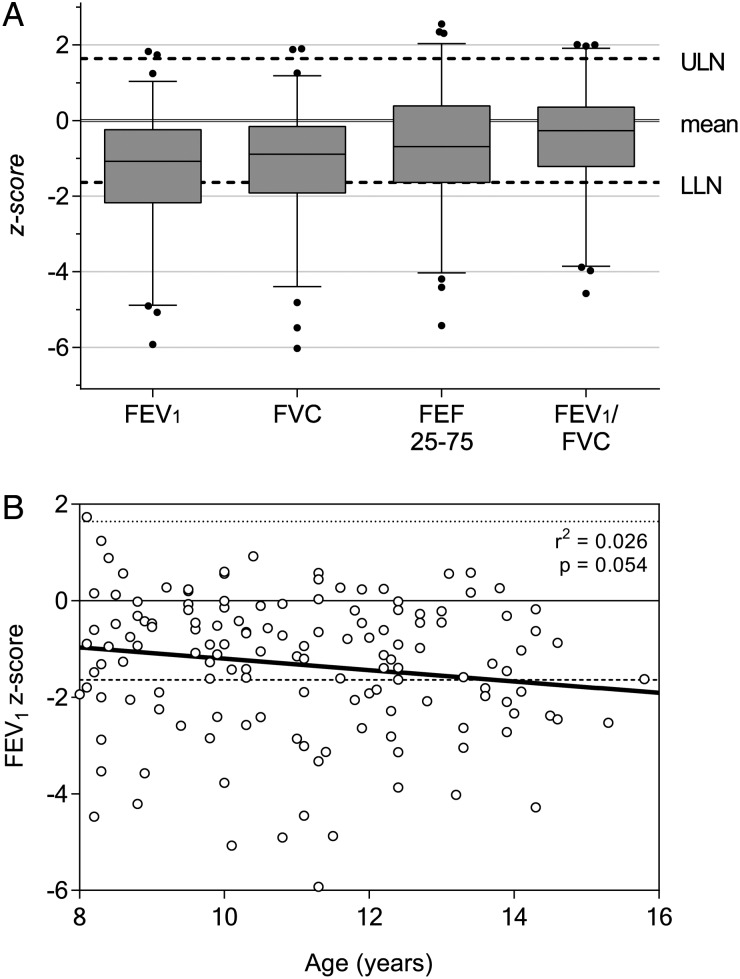
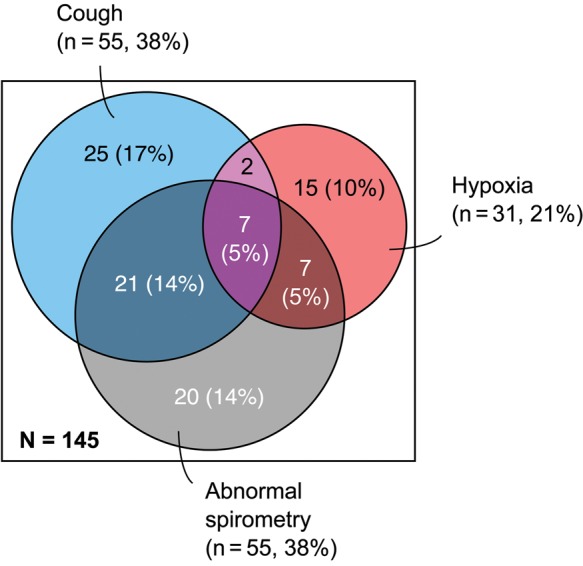
Results: One hundred sixty participants had a mean of age 11.1 (range, 8-16) years and 50.0% were female. Cough was present in 60 (37.5%) participants, and 55 (34.4%) had moderate or severe dyspnoea. Thirty-four (22.1%) participants had digital clubbing. Thirty-three (20.6%) participants were hypoxic at rest. One hundred eighteen (73.8%) of the children were receiving ART; median CD4 count was 698 cells/µL in these compared with 406 cells/µL in ART-naive individuals (P < .001). From 145 spirometry traces (90.6%), mean forced expiratory volume in 1 second (FEV1) and forced vital capacity (FVC) were 1.06 and 0.89 standard deviations below predicted mean, respectively. Twenty-one (14.5%) traces demonstrated obstructive defects and 26 (17.9%) reduced FVC. Lung function abnormality was not associated with any clinical findings. Of the 51 individuals with abnormal lung function, the mean increase in FEV1 after salbutamol was 3.8% (95% confidence interval, 0.02-7.53). "Tramlines" and ring shadows were seen on chest radiographs in over half of cases.
Conclusions: Symptoms of chronic lung disease were highly prevalent with 2 main clinical phenotypes: "cough" and "hypoxia". Lung function abnormalities are common, poorly responsive to bronchodilators, and apparent throughout the age range of our cohort. Pathological causes remain to be elucidated. Cough and hypoxic phenotypes could be a useful part of diagnostic algorithms if further validated.
Keywords: HIV; case definition; chronic lung disease; infectious disease transmission; respiratory function tests; vertical.
© The Author 2015. Published by Oxford University Press on behalf of the Pediatric Infectious Diseases Society.
Figures
References
-
- UNAIDS. 2014 progress report on the Global Plan. Geneva: UNAIDS; 2013.
-
- Sutcliffe CG, van Dijk JH, Bolton C et al. . Effectiveness of antiretroviral therapy among HIV-infected children in sub-Saharan Africa. Lancet Infect Dis 2008; 8:477–89. - PubMed
-
- Graham SM. Non-tuberculosis opportunistic infections and other lung diseases in HIV-infected infants and children. Int J Tuberc Lung Dis 2005; 9:592–602. - PubMed
-
- Lepage P, Van de Perre P, Van Vliet G et al. . Clinical and endocrinologic manifestations in perinatally human immunodeficiency virus type 1–Infected children aged 5 years or older. Am J Dis Child 1991; 145:1248–51. - PubMed
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
