

Cardiac Resynchronization Therapy in CKD Stage 4 Patients
- PMID: 26408549
- PMCID: PMC4594056
- DOI: 10.2215/CJN.00620115
Cardiac Resynchronization Therapy in CKD Stage 4 Patients
Abstract
Background and objectives: Cardiac resynchronization therapy (CRT) is a well established heart failure treatment that has shown to improve renal function. However, landmark CRT trials excluded patients with severe renal dysfunction. Therefore, this study evaluated the effect of CRT on renal function and long-term prognosis in patients with stage 4 CKD.
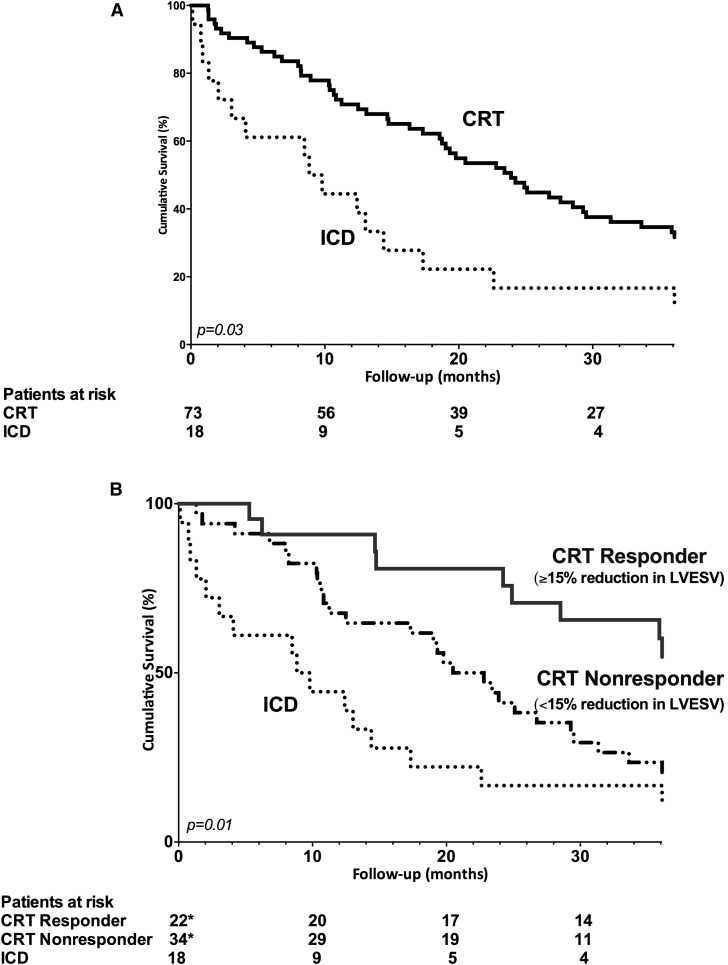
Design, setting, participants, & measurements: This study evaluated 73 consecutive CRT patients (71±10 years) with stage 4 CKD who underwent echocardiographic and renal function evaluation at baseline and 6-month follow-up between 2000 and 2012. As a control group, 18 patients with stage 4 CKD who received an implantable cardioverter defibrillator (ICD) were selected. CRT recipients with ≥15% reduction in left ventricular end-systolic volume at 6-month follow-up were classified as CRT responders. During long-term follow-up (median, 33 months), appropriate defibrillator therapy, heart failure hospitalizations, and all-cause mortality (combined end point) were recorded.
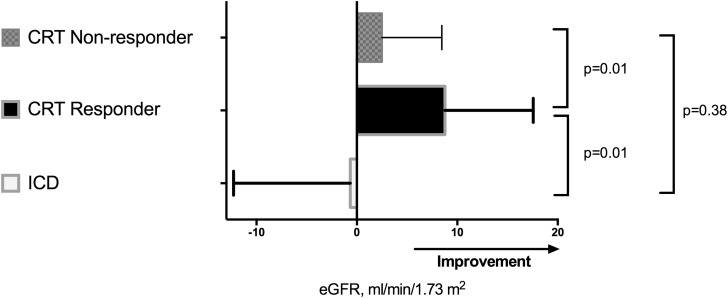
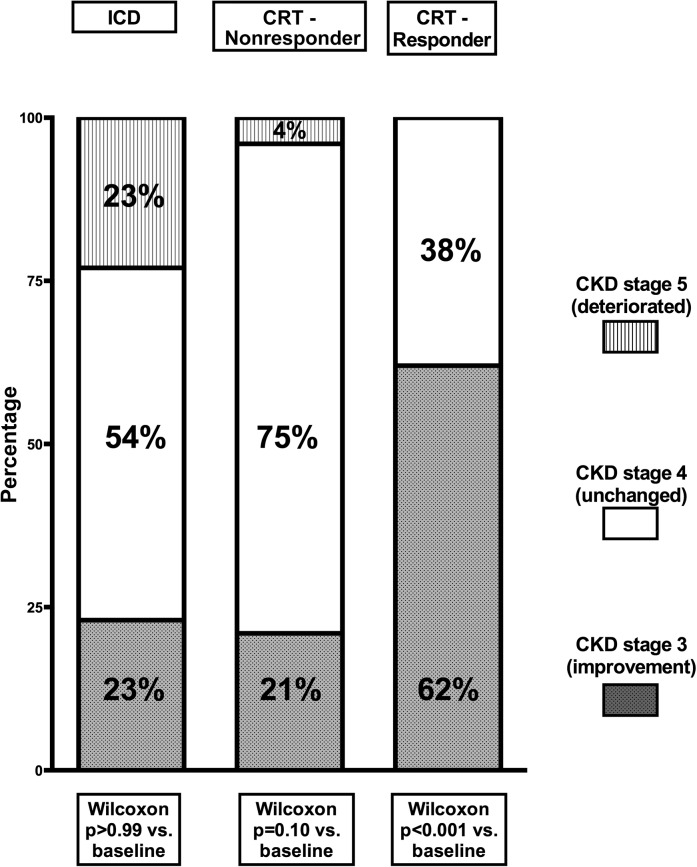
Results: At 6-month follow-up, a significant reduction in left ventricular end-systolic volume was observed in CRT patients compared with patients with ICD (from 159±78 to 145±78 ml in CRT patients and from 126±54 to 119±49 ml in ICD patients; P=0.05), and CRT response was observed in 22 patients (30%). Compared with ICD patients, eGFR improved among CRT patients (from 25±4 to 30±9 ml/min per 1.73 m(2); interaction time and group, P=0.04) and was more pronounced among CRT responders (25±3 to 34±9 ml/min per 1.73 m(2); P<0.001). The combined end point was observed in 17 ICD and 62 CRT patients. CRT patients showed superior survival compared with ICD patients (log-rank P=0.03). More importantly, CRT response was independently associated with improved survival free from the combined end point (hazard ratio, 0.51; 95% confidence interval, 0.27 to 0.98; P=0.04) after adjustment for clinical and echocardiographic parameters.
Conclusions: Response to CRT occurs in approximately 30% of patients with stage 4 CKD, which is less than in the average CRT population. CRT was associated with better clinical outcome, and particularly, CRT response was associated with improvement in eGFR and better long-term prognosis.
Keywords: chronic; chronic kidney disease; congestive heart failure; heart failure; renal function; survival.
Copyright © 2015 by the American Society of Nephrology.
Figures
Comment in
-
Cardiorenal Resynchronization Therapy: Strengthening the Heart and Kidneys.Clin J Am Soc Nephrol. 2015 Oct 7;10(10):1705-7. doi: 10.2215/CJN.09120815. Epub 2015 Sep 25. Clin J Am Soc Nephrol. 2015. PMID: 26408548 Free PMC article. No abstract available.
References
-
- McAlister FA, Ezekowitz J, Tonelli M, Armstrong PW: Renal insufficiency and heart failure: Prognostic and therapeutic implications from a prospective cohort study. Circulation 109: 1004–1009, 2004 - PubMed
-
- Hillege HL, Nitsch D, Pfeffer MA, Swedberg K, McMurray JJ, Yusuf S, Granger CB, Michelson EL, Ostergren J, Cornel JH, de Zeeuw D, Pocock S, van Veldhuisen DJ, Candesartan in Heart Failure: Assessment of Reduction in Mortality and Morbidity (CHARM) Investigators : Renal function as a predictor of outcome in a broad spectrum of patients with heart failure. Circulation 113: 671–678, 2006 - PubMed
-
- Damman K, van Deursen VM, Navis G, Voors AA, van Veldhuisen DJ, Hillege HL: Increased central venous pressure is associated with impaired renal function and mortality in a broad spectrum of patients with cardiovascular disease. J Am Coll Cardiol 53: 582–588, 2009 - PubMed
-
- Brignole M, Auricchio A, Baron-Esquivias G, Bordachar P, Boriani G, Breithardt OA, Cleland J, Deharo JC, Delgado V, Elliott PM, Gorenek B, Israel CW, Leclercq C, Linde C, Mont L, Padeletti L, Sutton R, Vardas PE, Zamorano JL, Achenbach S, Baumgartner H, Bax JJ, Bueno H, Dean V, Deaton C, Erol C, Fagard R, Ferrari R, Hasdai D, Hoes AW, Kirchhof P, Knuuti J, Kolh P, Lancellotti P, Linhart A, Nihoyannopoulos P, Piepoli MF, Ponikowski P, Sirnes PA, Tamargo JL, Tendera M, Torbicki A, Wijns W, Windecker S, Kirchhof P, Blomstrom-Lundqvist C, Badano LP, Aliyev F, Bänsch D, Baumgartner H, Bsata W, Buser P, Charron P, Daubert JC, Dobreanu D, Faerestrand S, Hasdai D, Hoes AW, Le Heuzey JY, Mavrakis H, McDonagh T, Merino JL, Nawar MM, Nielsen JC, Pieske B, Poposka L, Ruschitzka F, Tendera M, Van Gelder IC, Wilson CM, ESC Committee for Practice Guidelines (CPG) Document Reviewers : 2013 ESC Guidelines on cardiac pacing and cardiac resynchronization therapy: The Task Force on cardiac pacing and resynchronization therapy of the European Society of Cardiology (ESC). Developed in collaboration with the European Heart Rhythm Association (EHRA). Eur Heart J 34: 2281–2329, 2013 - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
