

Predictors of recurrence in the management of chordoid meningioma
- PMID: 26409888
- PMCID: PMC4684776
- DOI: 10.1007/s11060-015-1940-9
Predictors of recurrence in the management of chordoid meningioma
Erratum in
-
Erratum to: Predictors of recurrence in the management of chordoid meningioma.J Neurooncol. 2016 Jan;126(1):117. doi: 10.1007/s11060-015-1963-2. J Neurooncol. 2016. PMID: 26493739 No abstract available.
Abstract
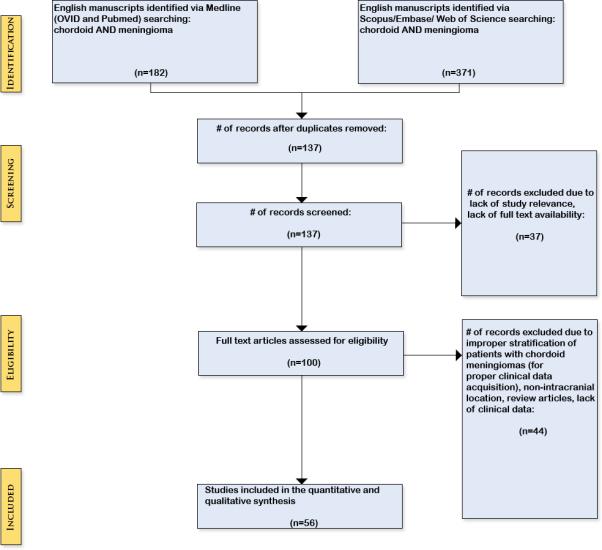
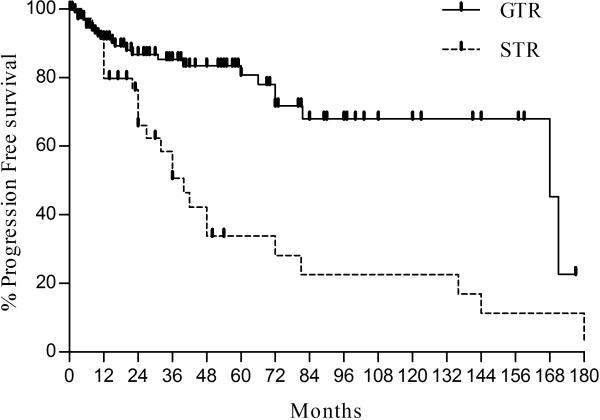
Management of chordoid meningiomas (CMs) is complicated by high rates of recurrence, particularly following subtotal resection. Optimal management is not established given the paucity of published experience. To identify prognostic factors for recurrence following resection, the authors conducted the largest systematic review of CMs to date. A comprehensive search on MEDLINE (OVID and Pubmed), Scopus, Embase, and Web of Science utilizing the search terms "chordoid" AND "meningioma" was performed to identify all reports of pathologically confirmed intracranial CMs. A total of 221 patients were included, comprising 120 females and 101 males. Mean age, MIB-1/Ki67, and tumor size was 45.5 years, 4.3% (range 0.1-26.6%), and 4.1 cm (range 0.8-10 cm), respectively. 5-, and 10- year progression free survival was 67.5 and 54.4%, respectively. Gross total resection (GTR) and subtotal resection was achieved in 172 and 48 patients, respectively. Adjuvant radiotherapy (RT) was given to 30 patients. Multivariate analysis found GTR was strongly correlated with decreased recurrence rates (HR 0.04, p = <0.0001), while higher MIB-1 labeling index (≥5 vs <5%) was associated with increased recurrence (HR 7.08; p = 0.016). Adjuvant RT, age, gender, and tumor location were not associated with recurrence. GTR resection is the strongest predictor of tumor control, and should be the goal to minimize local progression. Additionally, higher MIB-1 labeling was associated with increased rates of tumor recurrence. Tumors that are subtotally resected or demonstrate higher MIB-1 are at greater recurrence and warrant consideration for RT and close long term follow up.
Keywords: Atypical; Chordoid; Meningioma; Radiation therapy; Surgery.
Figures



References
-
- Kleihues P, Louis DN, Scheithauer BW, Rorke LB, Reifenberger G, Burger PC, Cavenee WK. The WHO classification of tumors of the nervous system. Journal of neuropathology and experimental neurology. 2002;61:215–225. discussion 226-219. - PubMed
-
- Couce ME, Aker FV, Scheithauer BW. Chordoid meningioma: a clinicopathologic study of 42 cases. The American journal of surgical pathology. 2000;24:899–905. - PubMed
-
- Epari S, Sharma MC, Sarkar C, Garg A, Gupta A, Mehta VS. Chordoid meningioma, an uncommon variant of meningioma: a clinicopathologic study of 12 cases. Journal of neuro-oncology. 2006;78:263–269. doi:10.1007/s11060-005-9092-y. - PubMed
-
- Kepes JJ, Chen WY, Connors MH, Vogel FS. “Chordoid” meningeal tumors in young individuals with peritumoral lymphoplasmacellular infiltrates causing systemic manifestations of the Castleman syndrome. A report of seven cases. Cancer. 1988;62:391–406. - PubMed
-
- Kozler P, Benes V, Netuka D, Kramar F, Hrabal P, Charvat F. Chordoid meningioma: presentation of two case reports, review of the literature, and plea for data standardisation. Journal of neuro-oncology. 2008;88:115–120. doi:10.1007/s11060-008-9541-5. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
