

Genomic Characterization of Brain Metastases Reveals Branched Evolution and Potential Therapeutic Targets
- PMID: 26410082
- PMCID: PMC4916970
- DOI: 10.1158/2159-8290.CD-15-0369
Genomic Characterization of Brain Metastases Reveals Branched Evolution and Potential Therapeutic Targets
Abstract
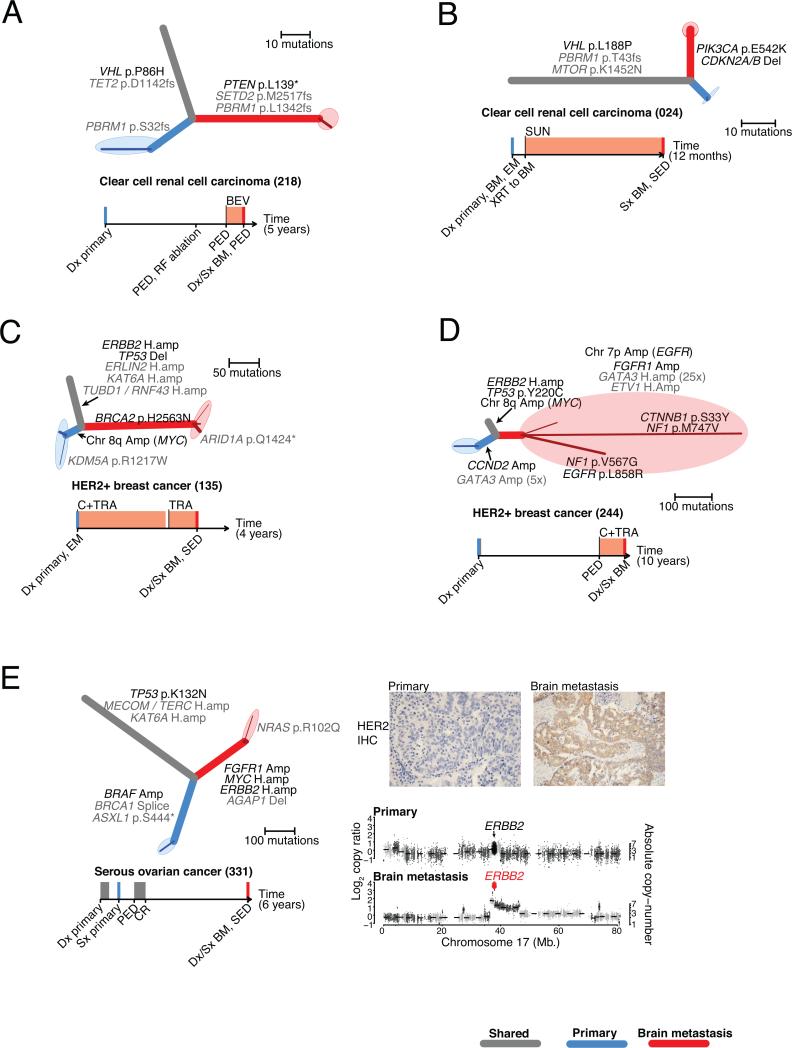
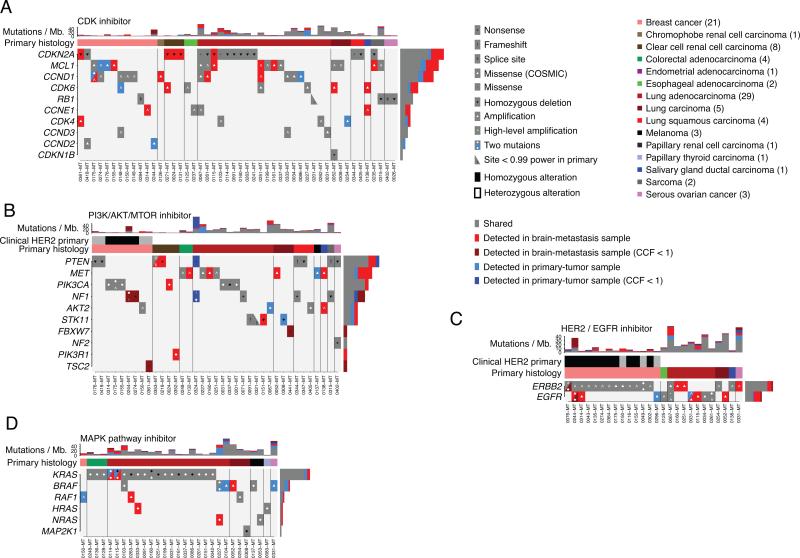
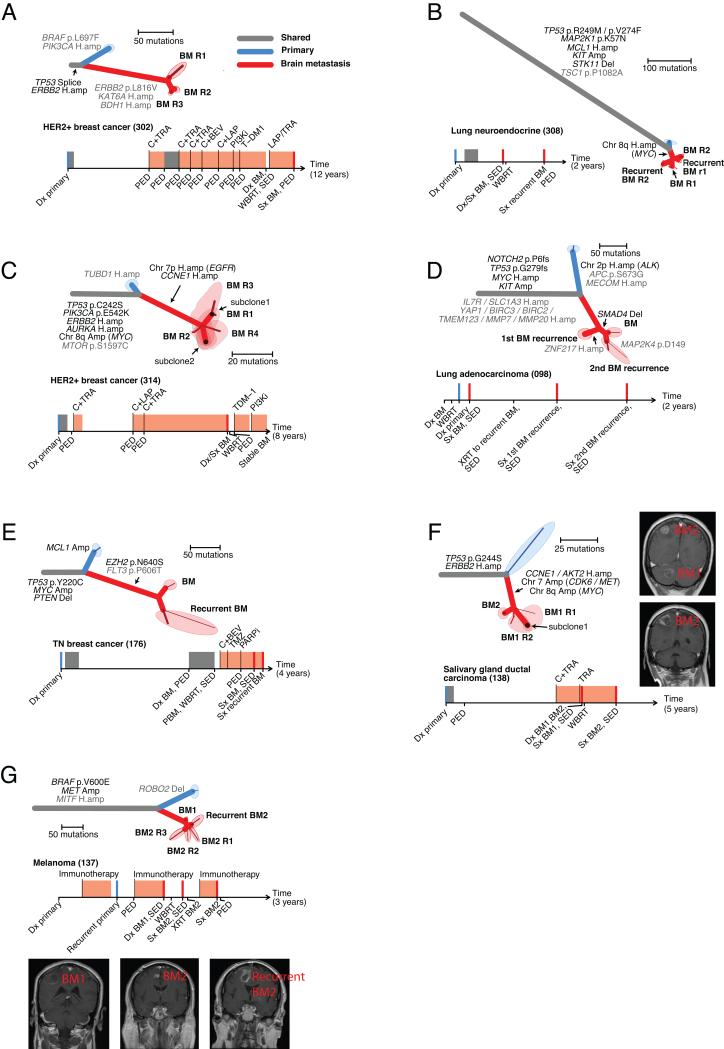
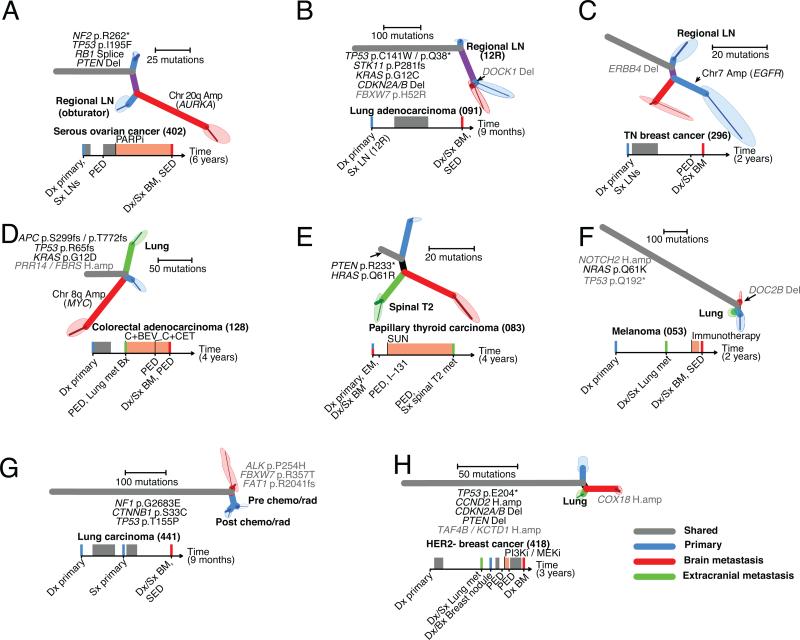
Brain metastases are associated with a dismal prognosis. Whether brain metastases harbor distinct genetic alterations beyond those observed in primary tumors is unknown. We performed whole-exome sequencing of 86 matched brain metastases, primary tumors, and normal tissue. In all clonally related cancer samples, we observed branched evolution, where all metastatic and primary sites shared a common ancestor yet continued to evolve independently. In 53% of cases, we found potentially clinically informative alterations in the brain metastases not detected in the matched primary-tumor sample. In contrast, spatially and temporally separated brain metastasis sites were genetically homogenous. Distal extracranial and regional lymph node metastases were highly divergent from brain metastases. We detected alterations associated with sensitivity to PI3K/AKT/mTOR, CDK, and HER2/EGFR inhibitors in the brain metastases. Genomic analysis of brain metastases provides an opportunity to identify potentially clinically informative alterations not detected in clinically sampled primary tumors, regional lymph nodes, or extracranial metastases.
Significance: Decisions for individualized therapies in patients with brain metastasis are often made from primary-tumor biopsies. We demonstrate that clinically actionable alterations present in brain metastases are frequently not detected in primary biopsies, suggesting that sequencing of primary biopsies alone may miss a substantial number of opportunities for targeted therapy.
©2015 American Association for Cancer Research.
Figures
References
-
- Brastianos PK, Curry WT, Oh KS. Clinical discussion and review of the management of brain metastases. J Natl Compr Canc Netw. 2013;11:1153–64. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
