

The inferior vena cava (IVC) syndrome as the initial manifestation of newly diagnosed gastric adenocarcinoma: a case report
- PMID: 26411979
- PMCID: PMC4584485
- DOI: 10.1186/s13256-015-0696-3
The inferior vena cava (IVC) syndrome as the initial manifestation of newly diagnosed gastric adenocarcinoma: a case report
Abstract
Introduction: Vena cava compression is a relatively rare initial manifestation of underlying malignancy. The superior vena cava syndrome, which is characterized by facial plethora, jugular venous distension, and arm swelling, is a well-known entity associated with bronchogenic carcinoma. Less common is the compression of the inferior vena cava. To the best of my knowledge, this is the first reported case of newly diagnosed gastric adenocarcinoma presenting initially as the inferior vena cava syndrome. The unique aspect about this case is that it highlights a rare presentation before diagnosis of gastric adenocarcinoma.
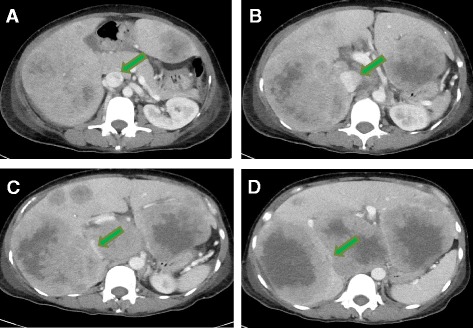
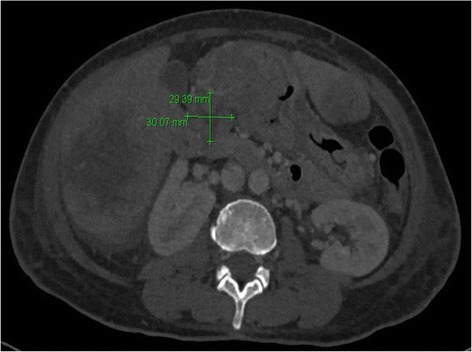
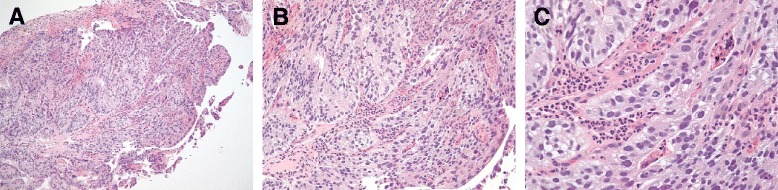
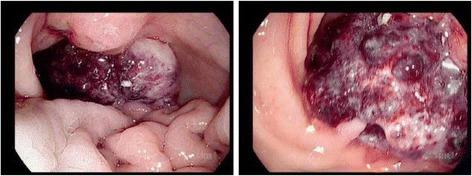
Case presentation: A 56-year-old Malaysian woman with a past medical history of iron deficiency anemia presented with lower extremity edema and progressive fatigue of 1 month's duration. She had significant worsening of leg swelling after standing for short periods of time. She also reported epigastric discomfort, which led to an additional workup, including computed tomography of the abdomen and pelvis. This revealed a 3cm×2.9cm mass in the stomach, extensive hepatic metastasis, and severe inferior vena cava compression. The patient was examined further with esophagogastroduodenoscopy, and a biopsy showed gastric adenocarcinoma.
Conclusions: This report describes a case of a patient with inferior vena cava syndrome as a unique presentation of previously undiagnosed stage IV gastric adenocarcinoma. Patients presenting with inferior vena cava syndrome should undergo prompt evaluation for underlying malignancies that have a predilection for hepatic metastasis. This case is important because earlier recognition of this syndrome can lead to earlier workup and thus detection of malignancy. Prompt initiation of treatment, including chemotherapy or vena cava stent placement, can result in improved patient outcome.
Figures
Similar articles
-
Budd-Chiari Syndrome and antithrombin III deficiency.Am J Clin Pathol. 1982 Aug;78(2):236-41. doi: 10.1093/ajcp/78.2.236. Am J Clin Pathol. 1982. PMID: 7102823
-
Intractable radicular and low back pain secondary inferior vena cava stenosis associated with Budd-Chiari syndrome: endovascular treatment with cava stenting: case report and review of the literature.Spine (Phila Pa 1976). 2006 May 20;31(12):E383-6. doi: 10.1097/01.brs.0000219516.54500.97. Spine (Phila Pa 1976). 2006. PMID: 16721285 Review.
-
Primary leiomyosarcoma of the inferior vena cava with Budd-Chiari syndrome.Acta Pathol Jpn. 1989 Jan;39(1):73-7. doi: 10.1111/j.1440-1827.1989.tb02405.x. Acta Pathol Jpn. 1989. PMID: 2652979 Review.
-
Leiomyosarcoma of the inferior vena cava causing Budd-Chiari syndrome--a case report.Angiology. 1993 Aug;44(8):673-6. doi: 10.1177/000331979304400814. Angiology. 1993. PMID: 8342886
-
Malignant inferior vena cava syndrome and congestive hepatic failure treated by venous stent placement.J Vasc Interv Radiol. 2012 Oct;23(10):1377-80. doi: 10.1016/j.jvir.2012.06.035. J Vasc Interv Radiol. 2012. PMID: 22999758
Cited by
-
S1Q3T3 Electrocardiographic Pattern in a Case of Colonic Ileus: A Case Report.Cureus. 2025 Mar 3;17(3):e79985. doi: 10.7759/cureus.79985. eCollection 2025 Mar. Cureus. 2025. PMID: 40177441 Free PMC article.
-
A Review of Gastric Cancer Research in Malaysia.Asian Pac J Cancer Prev. 2019 Jan 25;20(1):5-11. doi: 10.31557/APJCP.2019.20.1.5. Asian Pac J Cancer Prev. 2019. PMID: 30677863 Free PMC article. Review.
-
Inferior vena cava syndrome on skeletal scintigraphy secondary to metastatic prostate cancer.World J Nucl Med. 2020 Jul 2;19(3):324-326. doi: 10.4103/wjnm.WJNM_53_19. eCollection 2020 Jul-Sep. World J Nucl Med. 2020. PMID: 33354201 Free PMC article.
-
When Variants Collide: An Unusual Presentation of Metastatic Gastric Mixed Neuroendocrine-Non-Neuroendocrine Neoplasm.ACG Case Rep J. 2021 Apr 27;8(4):e00569. doi: 10.14309/crj.0000000000000569. eCollection 2021 Apr. ACG Case Rep J. 2021. PMID: 34476269 Free PMC article.
-
Multiple Myeloma With Retroperitoneal Extramedullary Plasmacytoma Causing Renal Failure and Obstructive Shock From Inferior Vena Cava Compression: A Case Report.Cureus. 2022 Nov 3;14(11):e31056. doi: 10.7759/cureus.31056. eCollection 2022 Nov. Cureus. 2022. PMID: 36475223 Free PMC article.
References
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
