

Associations of Protein Intake and Protein Source with Bone Mineral Density and Fracture Risk: A Population-Based Cohort Study
- PMID: 26412291
- PMCID: PMC5092173
- DOI: 10.1007/s12603-015-0544-6
Associations of Protein Intake and Protein Source with Bone Mineral Density and Fracture Risk: A Population-Based Cohort Study
Abstract
High dietary protein has been hypothesized to cause lower bone mineral density (BMD) and greater fracture risk. Previous results are conflicting and few studies have assessed potential differences related to differing protein sources.
Objective: To determine associations between total protein intake, and protein intake by source (dairy, non-dairy animal, plant) with BMD, BMD change, and incident osteoporotic fracture.
Design/setting: Prospective cohort study (Canadian Multicentre Osteoporosis Study). Participants/Measures: Protein intake was assessed as percent of total energy intake (TEI) at Year 2 (1997-99) using a food frequency questionnaire (N=6510). Participants were contacted annually to ascertain incident fracture. Total hip and lumbar spine BMD was measured at baseline and Year 5. Analyses were stratified by group (men 25-49 y, men 50+ y, premenopausal women 25-49 y, and postmenopausal women 50+ y) and adjusted for major confounders. Fracture analyses were limited to those 50+ y.
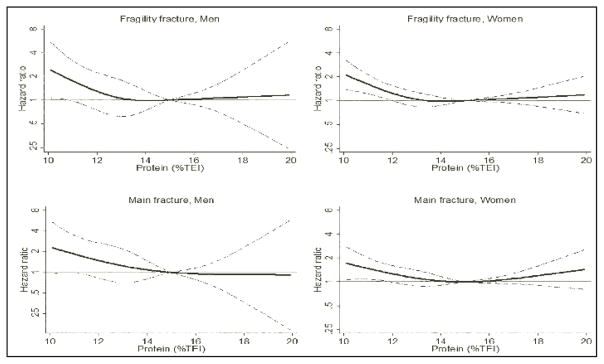
Results: Intakes of dairy protein (with adjustment for BMI) were positively associated with total hip BMD among men and women aged 50+ y, and in men aged 25-49. Among adults aged 50+ y, those with protein intakes of <12% TEI (women) and <11% TEI (men) had increased fracture risk compared to those with intakes of 15% TEI. Fracture risk did not significantly change as intake increased above 15% TEI, and was not significantly associated with protein source.
Conclusions: In contrast to hypothesized risk of high protein, we found that for adults 50+ y, low protein intake (below 15% TEI) may lead to increased fracture risk. Source of protein was a determinant of BMD, but not fracture risk.
Figures


References
-
- Burge R, Dawson-Hughes B, Solomon DH, Wong JB, King A, Tosteson A. Incidence and economic burden of osteoporosis-related fractures in the United States, 2005–2025. J Bone Miner Res. 2007;22:465–75. - PubMed
-
- Institute of Medicine,Panel on Macronutrients and Standing Committee on the Scientific Evaluation of Dietary Reference Intakes. Dietary reference intakes for energy, carbohydrate, fiber, fat, fatty acids, cholesterol, protein, and amino acids. Washington D.C: National Academies Press; 2005. pp. 769–879.
-
- Allen LH, Oddoye EA, Margen S. Protein-induced hypercalciuria: a longer term study. Am J Clin Nutr. 1979;32:741–9. - PubMed
-
- Cao JJ, Johnson LK, Hunt JR. A diet high in meat protein and potential renal acid load increases fractional calcium absorption and urinary calcium excretion without affecting markers of bone resorption or formation in postmenopausal women. J Nutr. 2011;141:391–7. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
