

Nivolumab versus Docetaxel in Advanced Nonsquamous Non-Small-Cell Lung Cancer
- PMID: 26412456
- PMCID: PMC5705936
- DOI: 10.1056/NEJMoa1507643
Nivolumab versus Docetaxel in Advanced Nonsquamous Non-Small-Cell Lung Cancer
Abstract
Background: Nivolumab, a fully human IgG4 programmed death 1 (PD-1) immune-checkpoint-inhibitor antibody, disrupts PD-1-mediated signaling and may restore antitumor immunity.
Methods: In this randomized, open-label, international phase 3 study, we assigned patients with nonsquamous non-small-cell lung cancer (NSCLC) that had progressed during or after platinum-based doublet chemotherapy to receive nivolumab at a dose of 3 mg per kilogram of body weight every 2 weeks or docetaxel at a dose of 75 mg per square meter of body-surface area every 3 weeks. The primary end point was overall survival.
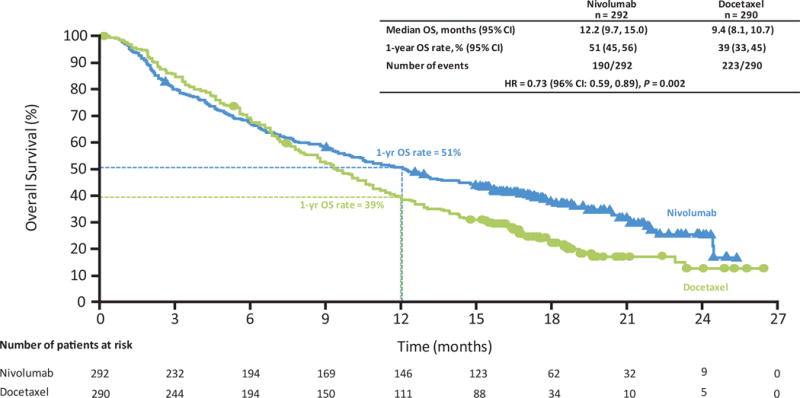
Results: Overall survival was longer with nivolumab than with docetaxel. The median overall survival was 12.2 months (95% confidence interval [CI], 9.7 to 15.0) among 292 patients in the nivolumab group and 9.4 months (95% CI, 8.1 to 10.7) among 290 patients in the docetaxel group (hazard ratio for death, 0.73; 96% CI, 0.59 to 0.89; P=0.002). At 1 year, the overall survival rate was 51% (95% CI, 45 to 56) with nivolumab versus 39% (95% CI, 33 to 45) with docetaxel. With additional follow-up, the overall survival rate at 18 months was 39% (95% CI, 34 to 45) with nivolumab versus 23% (95% CI, 19 to 28) with docetaxel. The response rate was 19% with nivolumab versus 12% with docetaxel (P=0.02). Although progression-free survival did not favor nivolumab over docetaxel (median, 2.3 months and 4.2 months, respectively), the rate of progression-free survival at 1 year was higher with nivolumab than with docetaxel (19% and 8%, respectively). Nivolumab was associated with even greater efficacy than docetaxel across all end points in subgroups defined according to prespecified levels of tumor-membrane expression (≥1%, ≥5%, and ≥10%) of the PD-1 ligand. Treatment-related adverse events of grade 3 or 4 were reported in 10% of the patients in the nivolumab group, as compared with 54% of those in the docetaxel group.
Conclusions: Among patients with advanced nonsquamous NSCLC that had progressed during or after platinum-based chemotherapy, overall survival was longer with nivolumab than with docetaxel. (Funded by Bristol-Myers Squibb; CheckMate 057 ClinicalTrials.gov number, NCT01673867.).
Figures



Comment in
-
Nivolumab--an effective second-line treatment for NSCLC.Nat Rev Clin Oncol. 2015 Dec;12(12):685. doi: 10.1038/nrclinonc.2015.184. Epub 2015 Oct 20. Nat Rev Clin Oncol. 2015. PMID: 26483299 No abstract available.
-
Nivolumab in Nonsquamous Non-Small-Cell Lung Cancer.N Engl J Med. 2016 Feb 4;374(5):493-4. doi: 10.1056/NEJMc1514790. N Engl J Med. 2016. PMID: 26840144 No abstract available.
-
Nivolumab in Nonsquamous Non-Small-Cell Lung Cancer.N Engl J Med. 2016 Feb 4;374(5):492-3. doi: 10.1056/NEJMc1514790. N Engl J Med. 2016. PMID: 26840145 No abstract available.
-
Nivolumab in Nonsquamous Non-Small-Cell Lung Cancer.N Engl J Med. 2016 Feb 4;374(5):493. doi: 10.1056/NEJMc1514790. N Engl J Med. 2016. PMID: 26840146 No abstract available.
-
The quest to extend the reach of checkpoint inhibitors in lung cancer.Nature. 2017 Dec 21;552(7685):S62-S63. doi: 10.1038/d41586-017-08700-9. Nature. 2017. PMID: 29293220 No abstract available.
-
Statistical Interpretation and Comparison of Waterfall Plots.JCO Clin Cancer Inform. 2023 Sep;7:e2300132. doi: 10.1200/CCI.23.00132. JCO Clin Cancer Inform. 2023. PMID: 37906725
References
-
- Fossella FV, DeVore R, Kerr RN, et al. Randomized phase III trial of docetaxel versus vinorelbine or ifosfamide in patients with advanced non-small-cell lung cancer previously treated with platinum-containing chemotherapy regimens. The TAX 320 Non-Small Cell Lung Cancer Study Group. J Clin oncol. 2000;18:2354–62. - PubMed
-
- Shepherd FA, Dancey J, Ramlau R, et al. Prospective randomized trial of docetaxel versus best supportive care in patients with non-small-cell lung cancer previously treated with platinum-based chemotherapy. J Clin Oncol. 2000;18:2095–103. - PubMed
-
- Taxotere (docetaxel) US Prescribing Information. 2010 May; Accessed March 23, 2015, at http://www.accessdata.fda.gov/drugsatfda_docs/label/2010/020449s059lbl.pdf.
-
- Hanna N, Shepherd FA, Fossella FV, et al. Randomized phase III trial of pemetrexed versus docetaxel in patients with non-small-cell lung cancer previously treated with chemotherapy. J Clin Oncol. 2004;22:1589–97. - PubMed
-
- Garassino MC, Martelli O, Broggini M, et al. Erlotinib versus docetaxel as second-line treatment of patients with advanced non-small-cell lung cancer and wild-type EGFR tumours (TAILOR): a randomised controlled trial. Lancet Oncol. 2013;14:981–88. - PubMed
Publication types
MeSH terms
Substances
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials