

Anomalous Origin of the Left Coronary Artery from the Pulmonary Artery: Diagnoses and Surgical Results in 12 Pediatric Patients
- PMID: 26413018
- PMCID: PMC4567127
- DOI: 10.14503/THIJ-13-3849
Anomalous Origin of the Left Coronary Artery from the Pulmonary Artery: Diagnoses and Surgical Results in 12 Pediatric Patients
Abstract
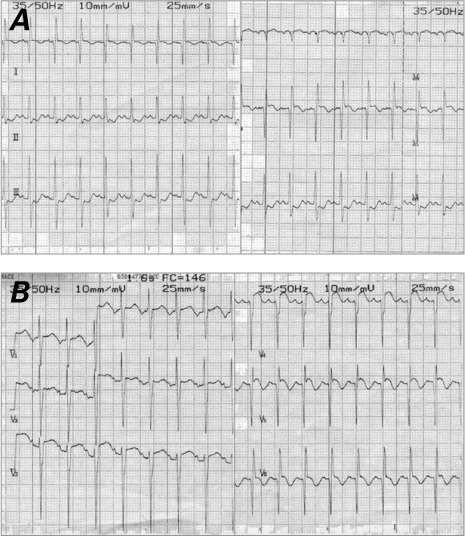
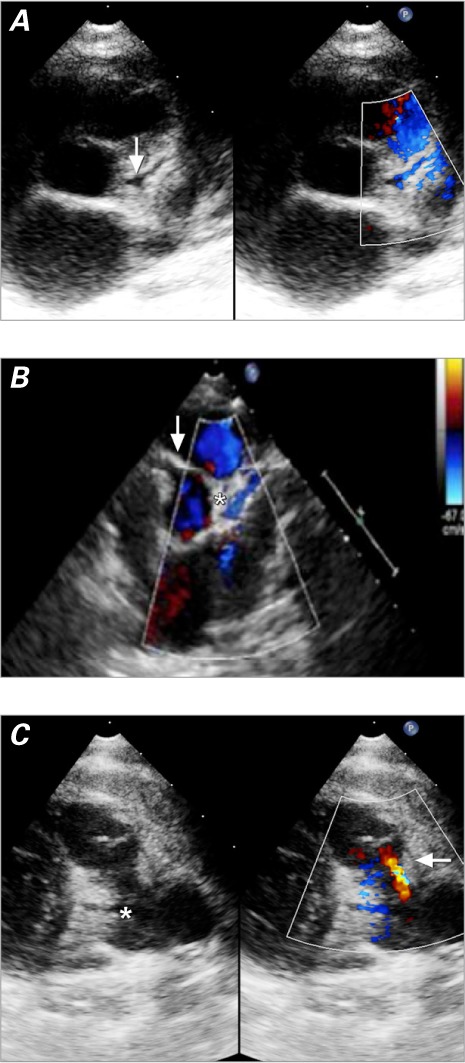
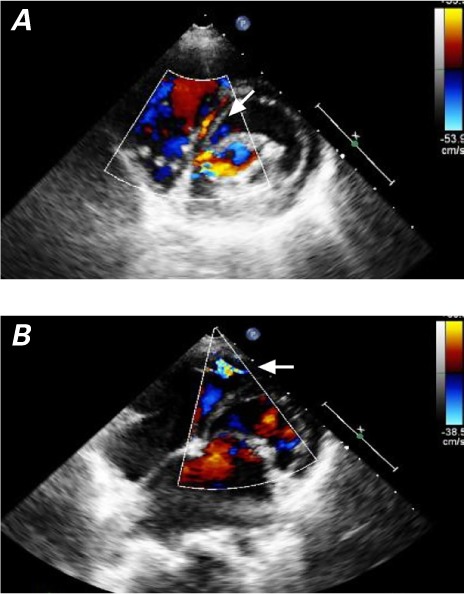
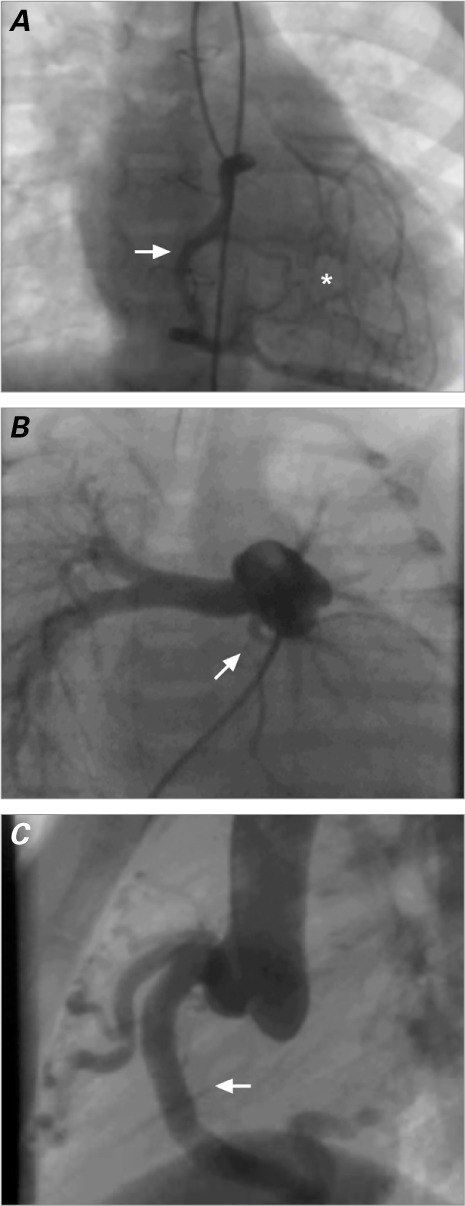
Anomalous origin of the left coronary artery from the pulmonary artery (ALCAPA) is a rare congenital condition. It responds well to early diagnosis and treatment, but otherwise the prognosis is poor. We present our case series of 12 patients (mean age, 2 ± 2.58 yr; age range, 2 mo-8 yr), emphasizing the diagnostic process and discussing our surgical results. The diagnosis of ALCAPA should be suspected in infants who have dilated cardiomyopathy with electrocardiographic changes that suggest ischemia, and in older children who have isolated mitral regurgitation. When clinical suspicion is high, the results of 2-dimensional echocardiography combined with color-flow Doppler studies in expert hands can establish the diagnosis, thus avoiding angiography in critically ill infants. The treatment of choice in our patients was transfer and reimplantation of the left coronary artery onto the ascending aorta. There were 2 deaths: both were infants in extremis who underwent emergency surgery. An older child with severe ventricular dysfunction was given mechanical ventricular assistance and then heart transplantation. As of this report, all 10 survivors remained well and asymptomatic.
Keywords: Abnormalities, multiple/diagnosis; cardiac surgical procedures/methods; cardiomyopathy, dilated/etiology/physiopathology; collateral circulation/physiology; coronary vessel anomalies/diagnosis/pathology/radiography/surgery; echocardiography, Doppler, color/methods; heart arrest/etiology; pulmonary artery/abnormalities/pathology; time factors; treatment outcome.
Figures
References
-
- Zemanek D, Veselka J. Coronary artery anomalies - a short review. Centr Eur J Med. 2007;2(2):140–53.
-
- Cowles RA, Berdon WE. Bland-White-Garland syndrome of anomalous left coronary artery arising from the pulmonary artery (ALCAPA): a historical review. Pediatr Radiol. 2007;37(9):890–5. - PubMed
-
- He XH, Li Y, Huang MR, Gao W, Li F, Yu ZQ et al. Anomalous origin of the left coronary artery from the pulmonary artery: report on 10 cases [in Chinese] Zhongguo Dang Dai Er Ke Za Zhi. 2007;9(1):25–7. - PubMed
-
- Walsh MA, Duff D, Oslizlok P, Redmond M, Walsh KP, Wood AE, Coleman DM. A review of 15-year experience with anomalous origin of the left coronary artery. Ir J Med Sci. 2008;177(2):127–30. - PubMed
-
- Tan X, Sun K, Li F, Zhang YQ, Wu LP. Clinical diagnosis of anomalous origin of the left coronary artery from the pulmonary artery in 22 cases [in Chinese] Zhonghua Er Ke Za Zhi. 2008;46(12):881–4. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Research Materials
