

Relationship between Right Ventricular Longitudinal Strain, Invasive Hemodynamics, and Functional Assessment in Pulmonary Arterial Hypertension
- PMID: 26413108
- PMCID: PMC4580699
- DOI: 10.4070/kcj.2015.45.5.398
Relationship between Right Ventricular Longitudinal Strain, Invasive Hemodynamics, and Functional Assessment in Pulmonary Arterial Hypertension
Erratum in
-
Erratum: Relationship between Right Ventricular Longitudinal Strain, Invasive Hemodynamics, and Functional Assessment in Pulmonary Arterial Hypertension.Korean Circ J. 2016 Mar;46(2):273. doi: 10.4070/kcj.2016.46.2.273. Epub 2016 Mar 21. Korean Circ J. 2016. PMID: 27014362 Free PMC article.
Abstract
Background and objectives: Right ventricular longitudinal strain (RVLS) is a new parameter of RV function. We evaluated the relationship of RVLS by speckle-tracking echocardiography with functional and invasive parameters in pulmonary arterial hypertension (PAH) patients.
Subjects and methods: Thirty four patients with World Health Organization group 1 PAH (29 females, mean age 45±13 years old). RVLS were analyzed with velocity vector imaging.
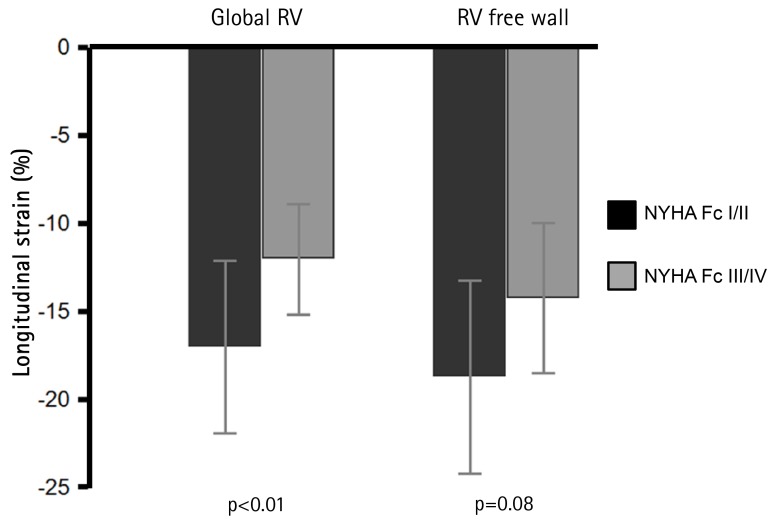
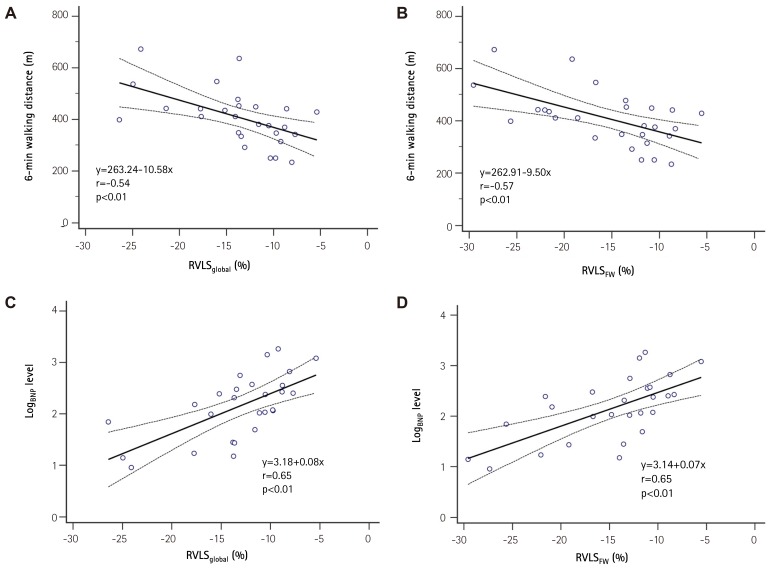
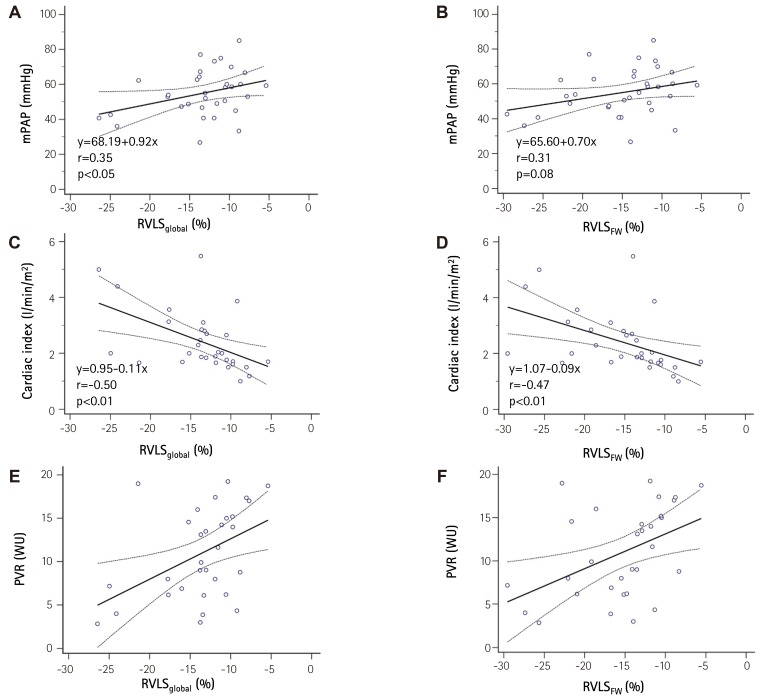
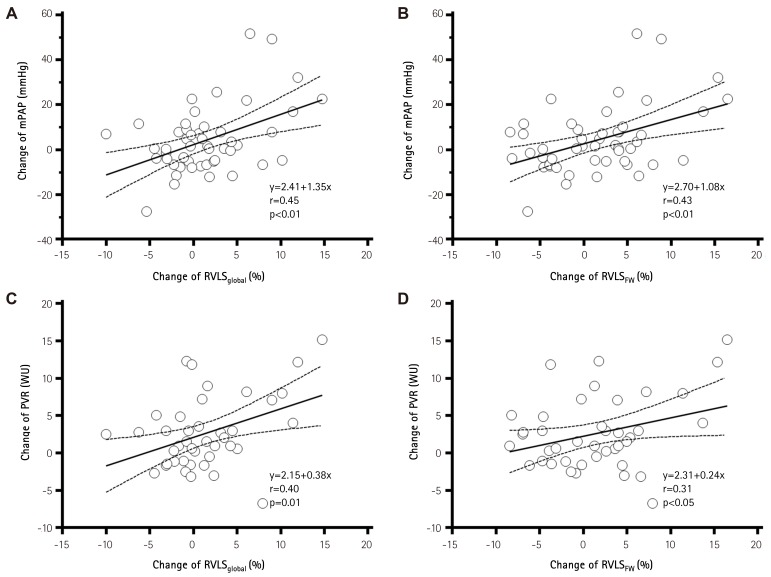
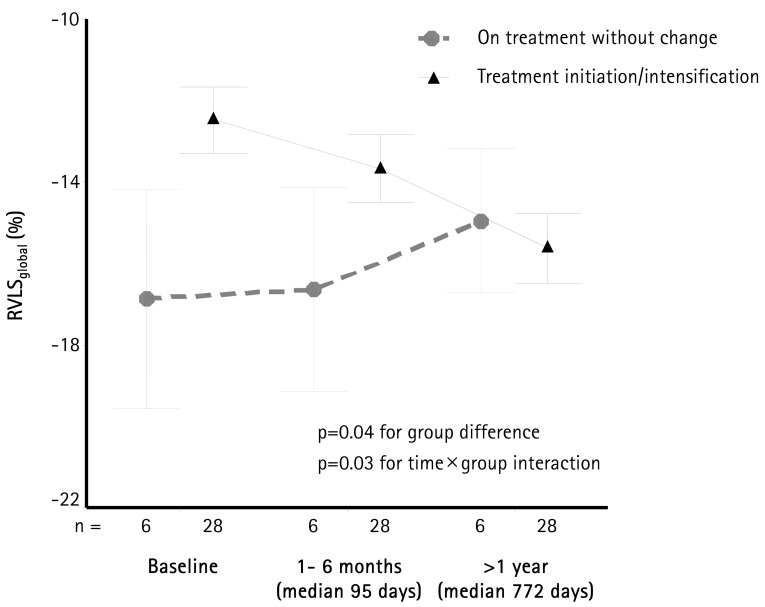
Results: Patients with advanced symptoms {New York Heart Association (NYHA) functional class III/IV} had impaired RVLS in global RV (RVLSglobal, -17±5 vs. -12±3%, p<0.01) and RV free wall (RVLSFW, -19±5 vs. -14±4%, p<0.01 to NYHA class I/II). Baseline RVLSglobal and RVLSFW showed significant correlation with 6-minute walking distance (r=-0.54 and r=-0.57, p<0.01 respectively) and logarithmic transformation of brain natriuretic peptide concentration (r=0.65 and r=0.65, p<0.01, respectively). These revealed significant correlations with cardiac index (r=-0.50 and r=-0.47, p<0.01, respectively) and pulmonary vascular resistance (PVR, r=0.45 and r=0.45, p=0.01, respectively). During a median follow-up of 33 months, 25 patients (74%) had follow-up examinations. Mean pulmonary arterial pressure (mPAP, 54±13 to 46±16 mmHg, p=0.03) and PVR (11±5 to 6±2 wood units, p<0.01) were significantly decreased with pulmonary vasodilator treatment. RVLSglobal (-12±5 to -16±5%, p<0.01) and RVLSFW (-14±5 to -18±5%, p<0.01) were significantly improved. The decrease of mPAP was significantly correlated with improvement of RVLSglobal (r=0.45, p<0.01) and RVLSFW (r=0.43, p<0.01). The PVR change demonstrated significant correlation with improvement of RVLSglobal (r=0.40, p<0.01).
Conclusion: RVLS correlates with functional and invasive hemodynamic parameters in PAH patients. Decrease of mPAP and PVR as a result of treatment was associated with improvement of RVLS.
Keywords: Familial primary pulmonary hypertension; Heart ventricles; Ventricular function, right.
Conflict of interest statement
The authors have no financial conflicts of interest.
Figures
References
-
- Humbert M, Sitbon O, Simonneau G. Treatment of pulmonary arterial hypertension. N Engl J Med. 2004;351:1425–1436. - PubMed
-
- Bogaard HJ, Abe K, Vonk Noordegraaf A, Voelkel NF. The right ventricle under pressure: cellular and molecular mechanisms of right-heart failure in pulmonary hypertension. Chest. 2009;135:794–804. - PubMed
-
- D'Alonzo GE, Barst RJ, Ayres SM, et al. Survival in patients with primary pulmonary hypertension. Results from a national prospective registry. Ann Intern Med. 1991;115:343–349. - PubMed
-
- Barst RJ, Rubin LJ, Long WA, et al. A comparison of continuous intravenous epoprostenol (prostacyclin) with conventional therapy for primary pulmonary hypertension. N Engl J Med. 1996;334:296–301. - PubMed
-
- Channick RN, Simonneau G, Sitbon O, et al. Effects of the dual endothelin-receptor antagonist bosentan in patients with pulmonary hypertension: a randomised placebo-controlled study. Lancet. 2001;358:1119–1123. - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials
