

Spontaneous Involution of a Presumably Rathke's Cleft Cyst in a Patient with Slight Subclinical Hypopituitarism: A Case Report and Review of the Literature
- PMID: 26413367
- PMCID: PMC4564632
- DOI: 10.1155/2015/971364
Spontaneous Involution of a Presumably Rathke's Cleft Cyst in a Patient with Slight Subclinical Hypopituitarism: A Case Report and Review of the Literature
Abstract
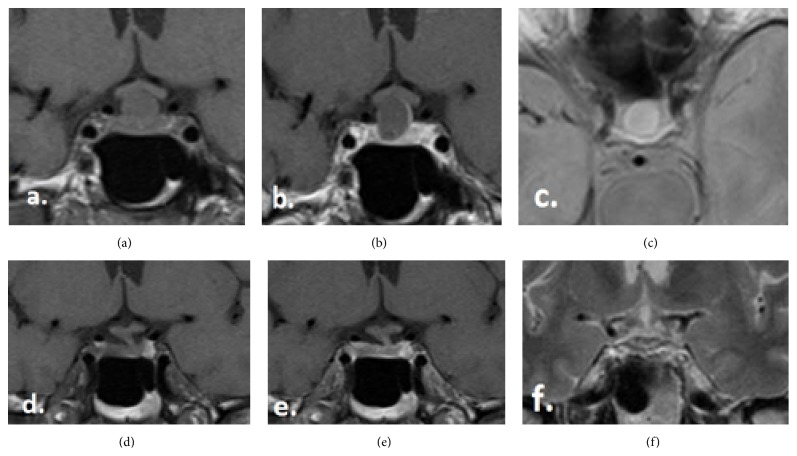
Rathke cleft cyst is described as benign intrasellar cyst. They are mostly small and asymptomatic; they may become large enough to cause symptoms by compression of intrasellar or suprasellar structures. We report on a case of spontaneous regression of a symptomatic RCC with subsequent recovery of preexisting endocrine dysfunction and resolution of headaches. A 60-year-old man complained about headaches. Laboratory investigation revealed a partial hypopituitarism with a slight central hypothyroidism without need for substitution. An MRI study showed a cystic, T2-hyperintense, sellar lesion compatible with a RCC. At one year follow-up, the patient had no complaints and the hormone work-up revealed a regression of the previous slight hypopituitarism. The MRI study showed a complete regression of the cystic lesion and a normal sized and shaped pituitary gland. The spontaneous regression of cystic sellar lesions is rare. The exact mechanism of the possible spontaneous involution of RCC is until now not well understood. However, spontaneous regression is possible and justifies the conservative therapy with regular clinical and radiological follow-up for asymptomatic patients or patients with symptoms not caused by the mass effect of these lesions.
Figures
References
-
- Zada G. Rathke cleft cysts: a review of clinical and surgical management. Neurosurgical Focus. 2011;31(1, article E1) - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources
