

Immune and Inflammatory Cell Composition of Human Lung Cancer Stroma
- PMID: 26413839
- PMCID: PMC4587668
- DOI: 10.1371/journal.pone.0139073
Immune and Inflammatory Cell Composition of Human Lung Cancer Stroma
Abstract
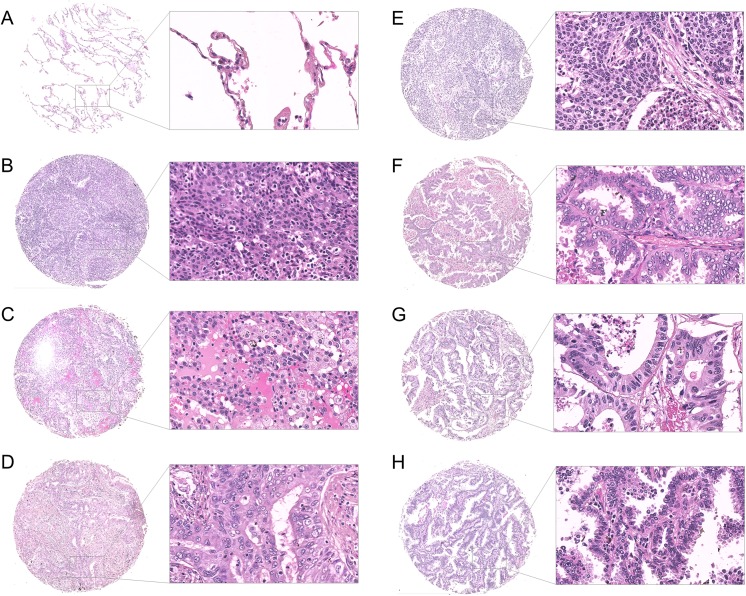
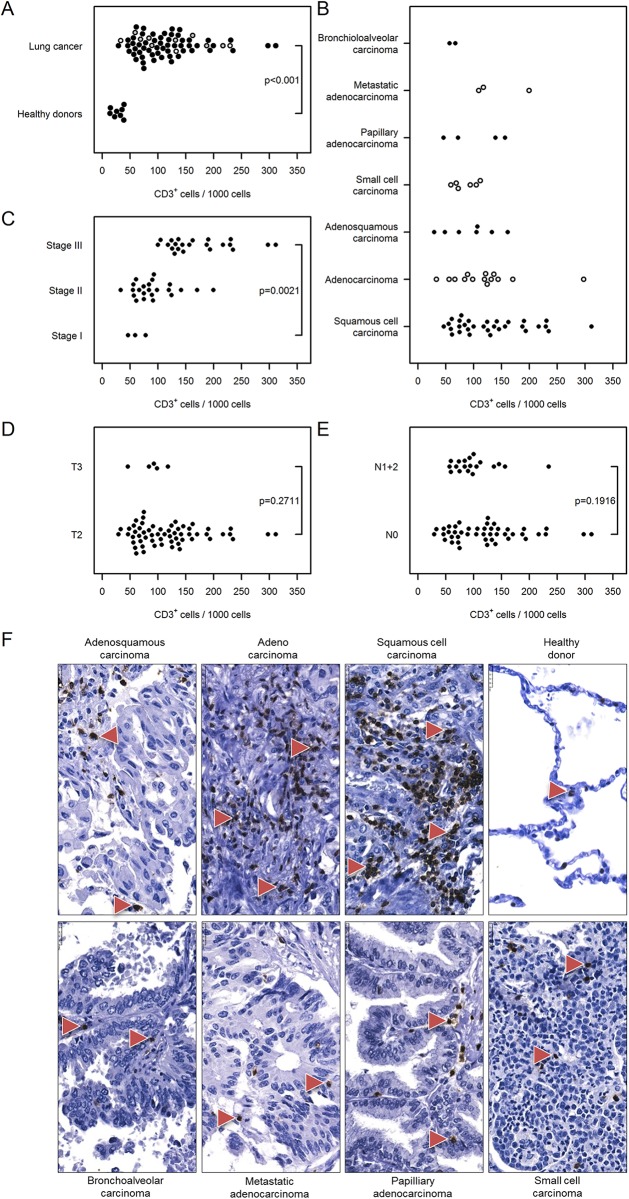
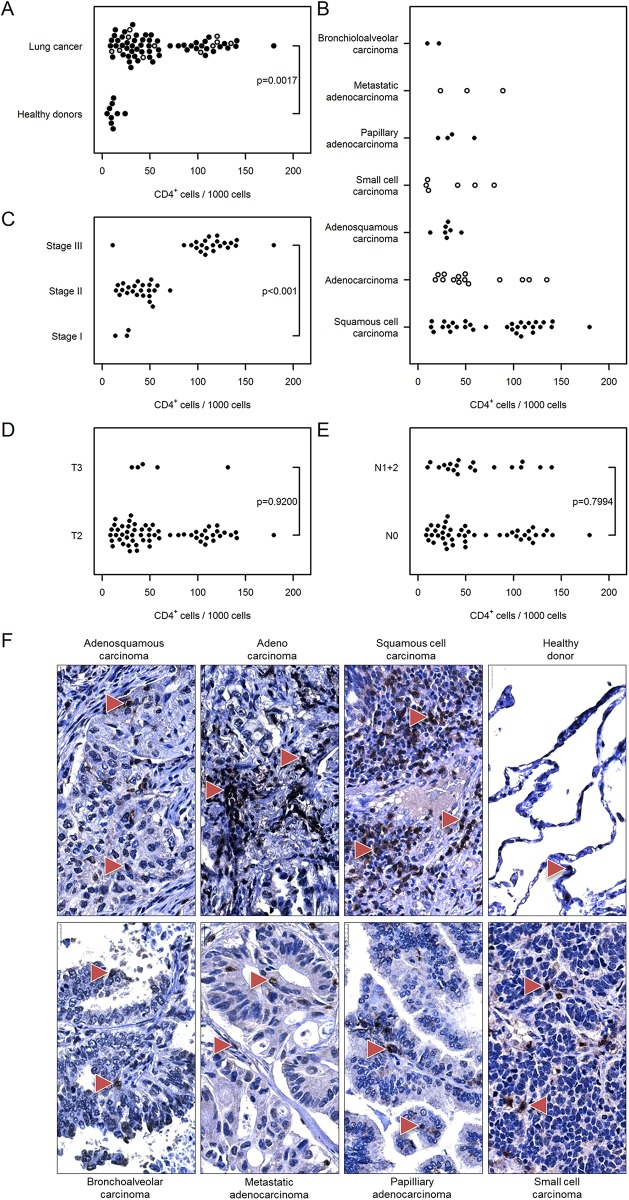
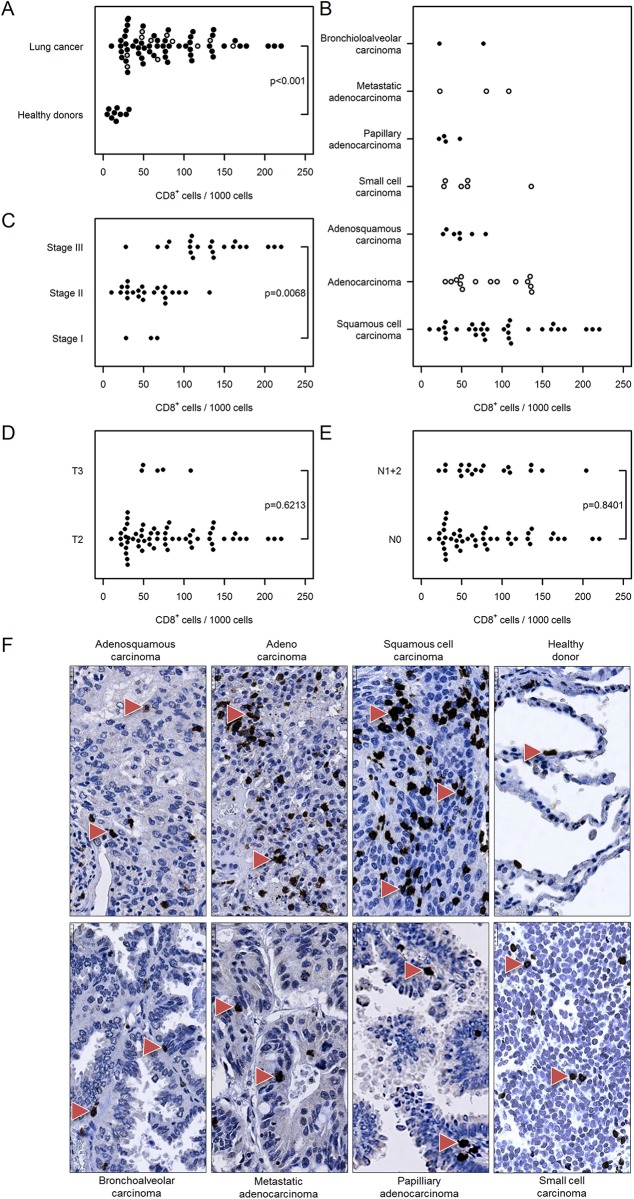
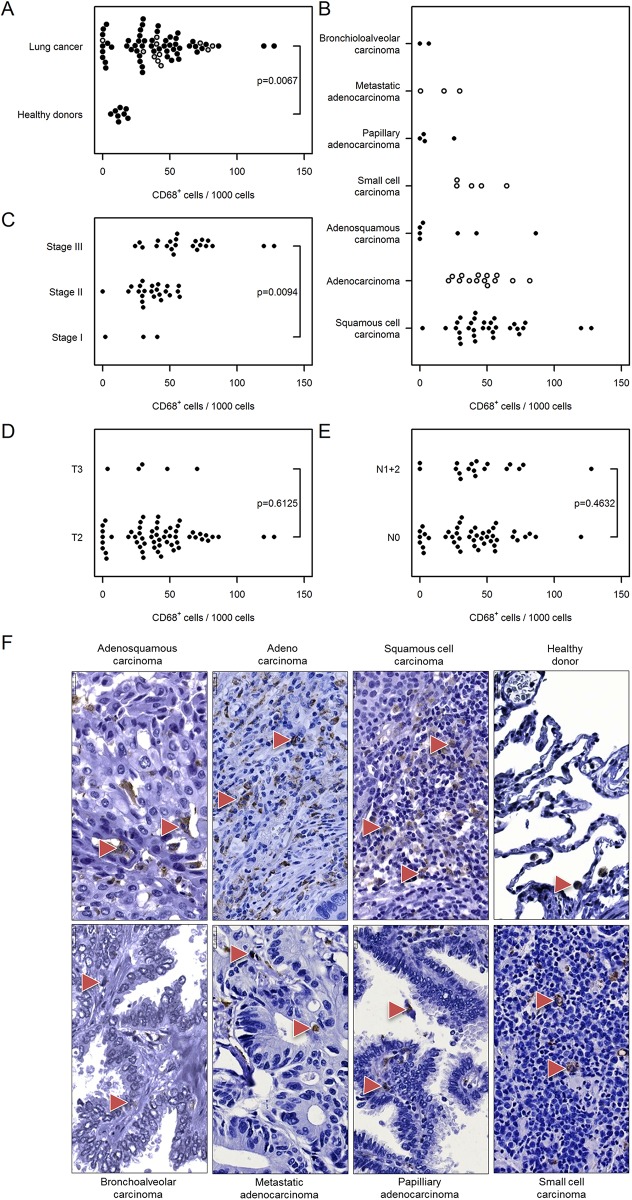
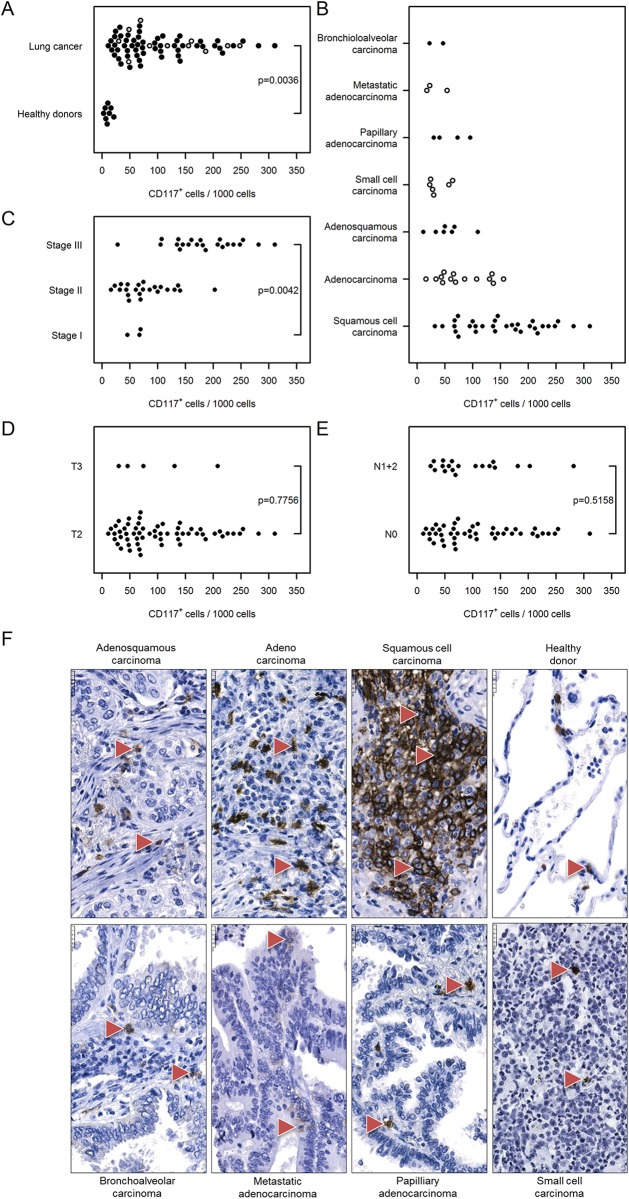
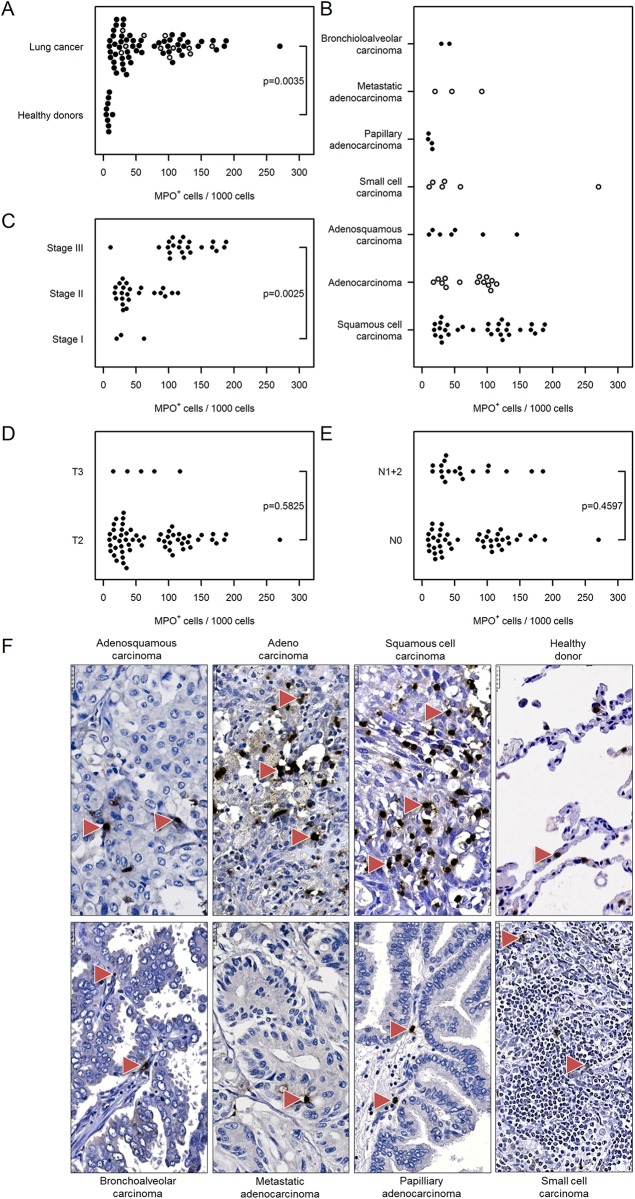
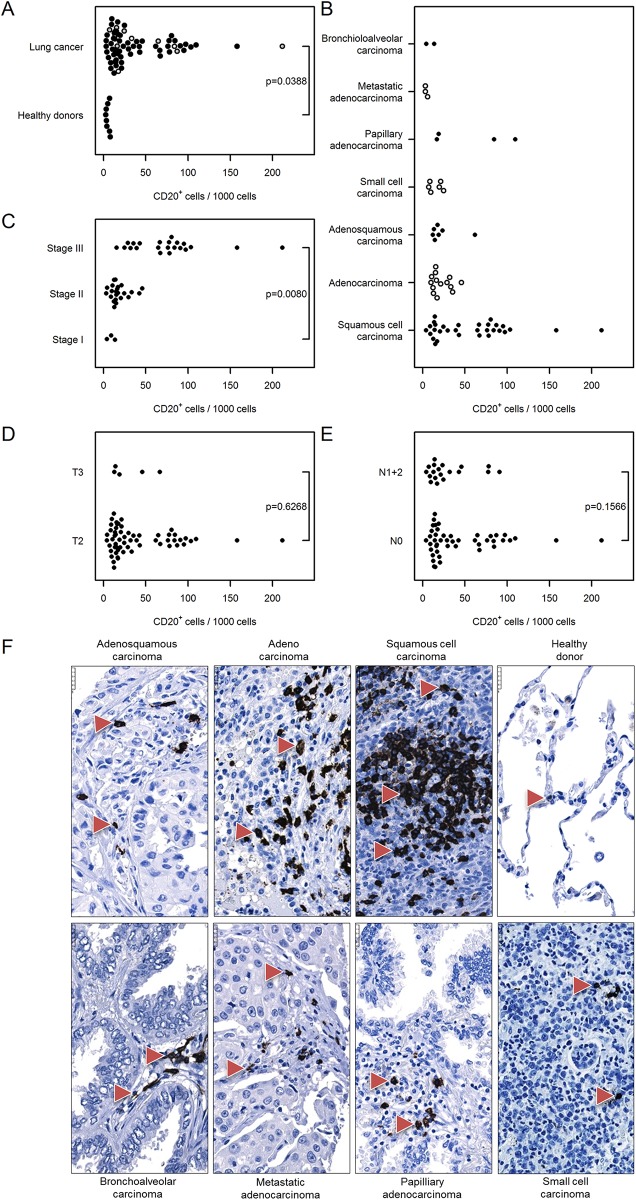
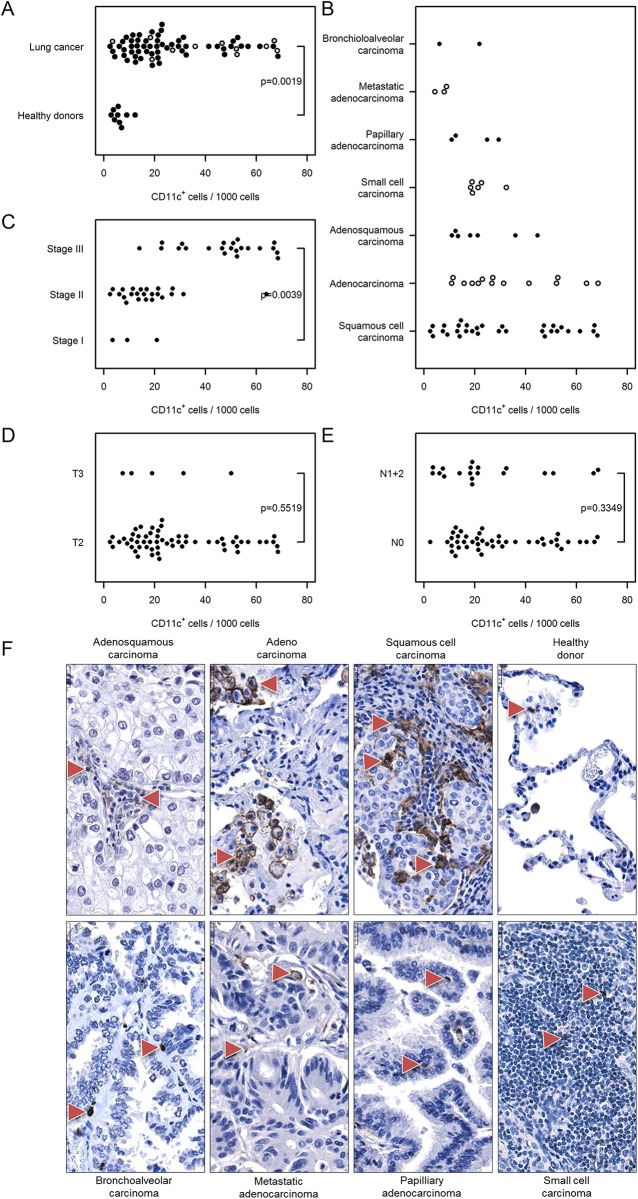
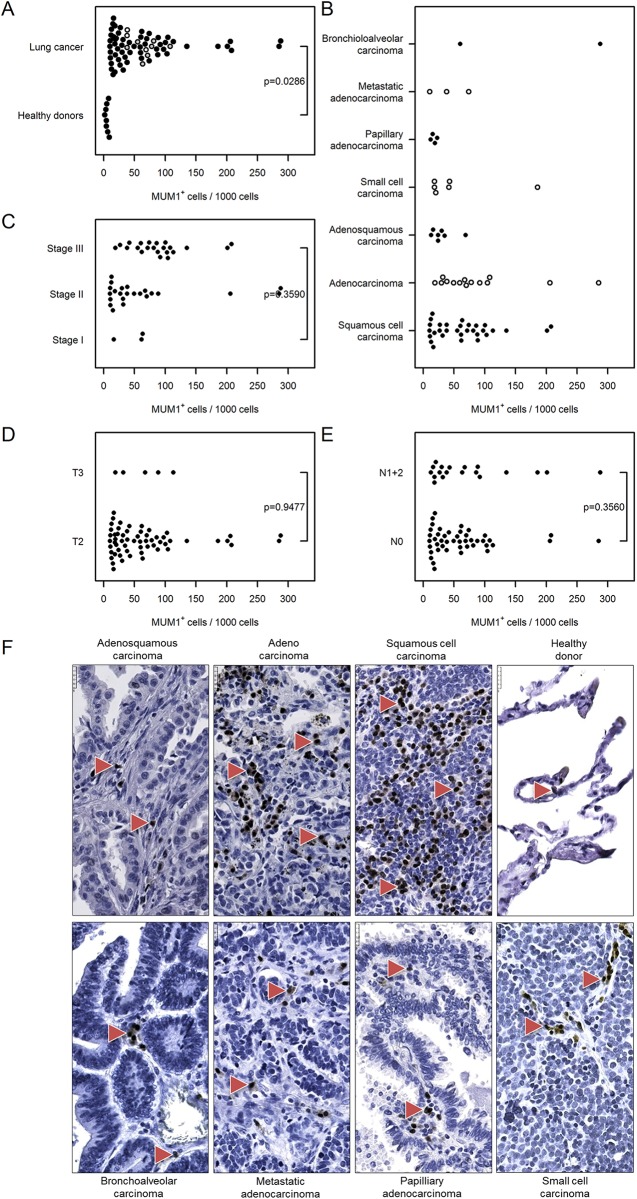
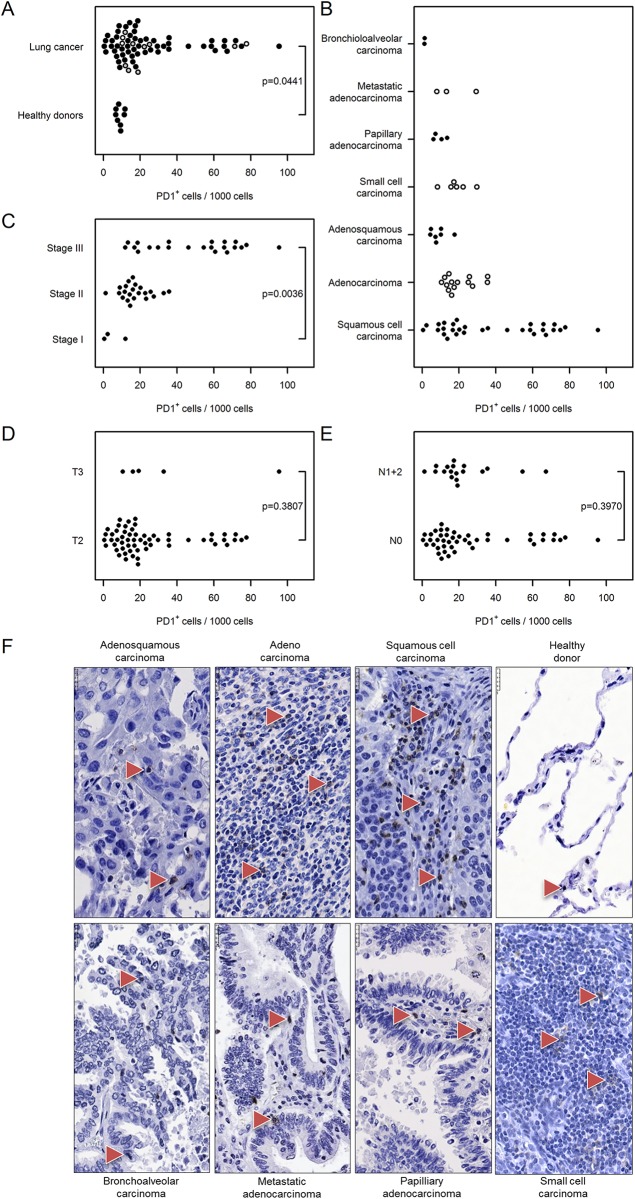
Recent studies indicate that the abnormal microenvironment of tumors may play a critical role in carcinogenesis, including lung cancer. We comprehensively assessed the number of stromal cells, especially immune/inflammatory cells, in lung cancer and evaluated their infiltration in cancers of different stages, types and metastatic characteristics potential. Immunohistochemical analysis of lung cancer tissue arrays containing normal and lung cancer sections was performed. This analysis was combined with cyto-/histomorphological assessment and quantification of cells to classify/subclassify tumors accurately and to perform a high throughput analysis of stromal cell composition in different types of lung cancer. In human lung cancer sections we observed a significant elevation/infiltration of total-T lymphocytes (CD3+), cytotoxic-T cells (CD8+), T-helper cells (CD4+), B cells (CD20+), macrophages (CD68+), mast cells (CD117+), mononuclear cells (CD11c+), plasma cells, activated-T cells (MUM1+), B cells, myeloid cells (PD1+) and neutrophilic granulocytes (myeloperoxidase+) compared with healthy donor specimens. We observed all of these immune cell markers in different types of lung cancers including squamous cell carcinoma, adenocarcinoma, adenosquamous cell carcinoma, small cell carcinoma, papillary adenocarcinoma, metastatic adenocarcinoma, and bronchioloalveolar carcinoma. The numbers of all tumor-associated immune cells (except MUM1+ cells) in stage III cancer specimens was significantly greater than those in stage I samples. We observed substantial stage-dependent immune cell infiltration in human lung tumors suggesting that the tumor microenvironment plays a critical role during lung carcinogenesis. Strategies for therapeutic interference with lung cancer microenvironment should consider the complexity of its immune cell composition.
Conflict of interest statement
Figures
References
-
- Lorenz J, Friedberg T, Paulus R, Oesch F, Ferlinz R. Oncogene overexpression in non-small-cell lung cancer tissue: prevalence and clinicopathological significance. Clin Investig. 1994;72(2):156–63. . - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
