

Influence of the Metaboreflex on Pulmonary Vascular Capacitance in Heart Failure
- PMID: 26414317
- PMCID: PMC4760838
- DOI: 10.1249/MSS.0000000000000775
Influence of the Metaboreflex on Pulmonary Vascular Capacitance in Heart Failure
Abstract
Purpose: An impaired metaboreflex is associated with abnormal ventilatory and peripheral vascular function in heart failure (HF), whereas its influence on cardiac function or pulmonary vascular pressure remains unclear. We aimed to assess whether metabolite-sensitive neural feedback (metaboreflex) from locomotor muscles via postexercise regional circulatory occlusion (RCO) attenuates pulmonary vascular capacitance (GXCAP) and/or circulatory power (CircP) in patients with HF.
Methods: Eleven patients with HF (NYHA class, I/II; ages, 51 ± 15 yr; ejection fraction, 32% ± 9%) and 11 age- and gender-matched controls (ages, 43 ± 9 yr) completed three cycling sessions (4 min, 60% peak oxygen uptake (V˙O2)). Session 1 was a control trial including normal recovery (NR). Session 2 or 3 included bilateral upper thigh pressure tourniquets inflated suprasystolic at end of exercise (RCO) for 2-min recovery with or without inspired CO2 (RCO + CO2) (randomized). Mean arterial pressure, HR, and V˙O2 were continuously measured. Estimates of central hemodynamics; CircP = (V˙O2 × mean arterial pressure)/weight; oxygen pulse index (O2pulseI = (V˙O2/HR)/body surface area); and GXCAP = O2pulseI × end-tidal partial pressure CO2 were calculated.
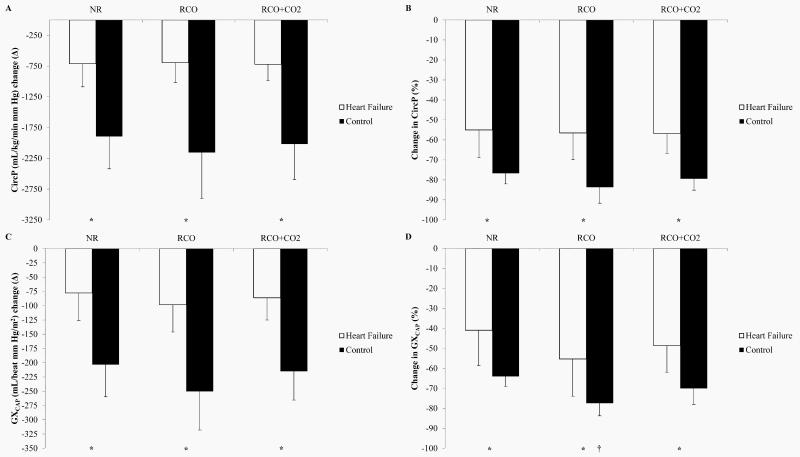
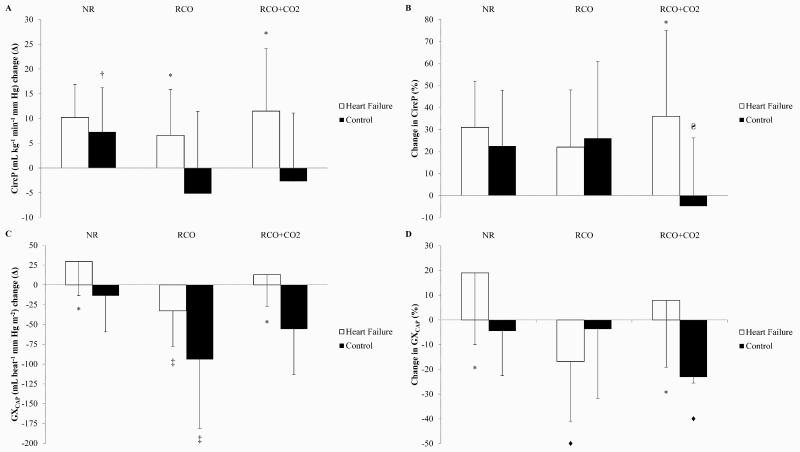
Results: At rest and end of exercise, CircP and GXCAP were lower in HF versus those in controls (P < 0.05), with no differences between transients (P > 0.05). At 2-min recovery, GXCAP was lower during RCO versus that during NR in both groups (72 ± 23 vs 98 ± 20 and 73 ± 34 vs 114 ± 35 mL·beat·mm Hg·m, respectively; P < 0.05), whereas CircP did not differ between transients (P > 0.05). Differences (% and Δ) between baseline and 2-min recovery among transients suggest that metaboreflex attenuates GXCAP in HF. Differences (% and Δ) between baseline and 2-min recovery among transients suggest that metaboreflex may attenuate CircP in controls.
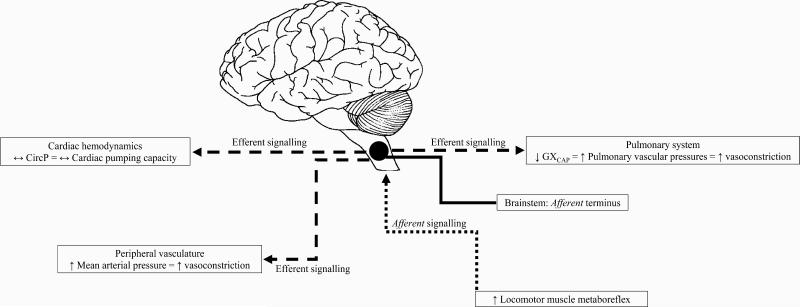
Conclusions: The present observations suggest that locomotor muscle metaboreflex activation may influence CircP in controls but not in HF. However, metaboreflex activation may evoke decreases in GXCAP (increased pulmonary vascular pressures) in HF and controls.
Figures
References
-
- Abramson SV, Burke JF, Kelly JJ, et al. Pulmonary hypertension predicts mortality and morbidity in patients with dilated cardiomyopathy. Annals of internal medicine. 1992;116(11):888–95. - PubMed
-
- Aronson D, Eitan A, Dragu R, Burger AJ. Relationship between reactive pulmonary hypertension and mortality in patients with acute decompensated heart failure. Circulation. Heart failure. 2011;4(5):644–50. - PubMed
-
- Butler J, Chomsky DB, Wilson JR. Pulmonary hypertension and exercise intolerance in patients with heart failure. Journal of the American College of Cardiology. 1999;34(6):1802–6. - PubMed
-
- Cohen-Solal A, Tabet JY, Logeart D, Bourgoin P, Tokmakova M, Dahan M. A non-invasively determined surrogate of cardiac power ('circulatory power') at peak exercise is a powerful prognostic factor in chronic heart failure. Eur Heart J. 2002;23(10):806–14. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
