

Effects of Multiple Ventilation Courses and Duration of Mechanical Ventilation on Respiratory Outcomes in Extremely Low-Birth-Weight Infants
- PMID: 26414549
- PMCID: PMC6445387
- DOI: 10.1001/jamapediatrics.2015.2401
Effects of Multiple Ventilation Courses and Duration of Mechanical Ventilation on Respiratory Outcomes in Extremely Low-Birth-Weight Infants
Abstract
Importance: Extubation failure is common in extremely preterm infants. The current paucity of data on the adverse long-term respiratory outcomes associated with reinitiation of mechanical ventilation prevents assessment of the risks and benefits of a trial of extubation in this population.
Objective: To evaluate whether exposure to multiple courses of mechanical ventilation increases the risk of adverse respiratory outcomes before and after adjustment for the cumulative duration of mechanical ventilation.
Design, setting, and participants: We performed a retrospective cohort study of extremely low-birth-weight (ELBW; birth weight <1000 g) infants born from January 1, 2006, through December 31, 2012, who were receiving mechanical ventilation. Analysis was conducted between November 2014 and February 2015. Data were obtained from the Alere Neonatal Database.
Exposures: The primary study exposures were the cumulative duration of mechanical ventilation and the number of ventilation courses.
Main outcomes and measures: The primary outcome was bronchopulmonary dysplasia (BPD) among survivors. Secondary outcomes were death, use of supplemental oxygen at discharge, and tracheostomy.
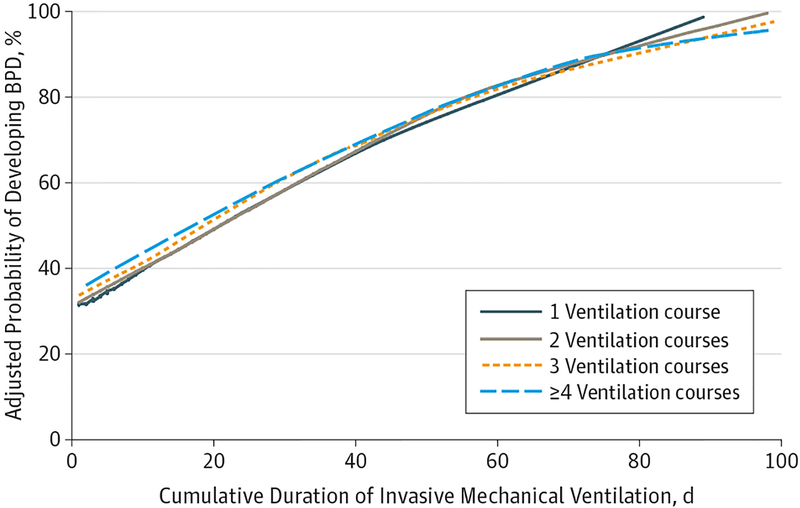
Results: We identified 3343 ELBW infants, of whom 2867 (85.8%) survived to discharge. Among the survivors, 1695 (59.1%) were diagnosed as having BPD, 856 (29.9%) received supplemental oxygen at discharge, and 31 (1.1%) underwent tracheostomy. Exposure to a greater number of mechanical ventilation courses was associated with a progressive increase in the risk of BPD and use of supplemental oxygen at discharge. Compared with a single ventilation course, the adjusted odds ratios for BPD ranged from 1.88 (95% CI, 1.54-2.31) among infants with 2 ventilation courses to 3.81 (95% CI, 2.88-5.04) among those with 4 or more courses. After adjustment for the cumulative duration of mechanical ventilation, the odds of BPD were only increased among infants exposed to 4 or more ventilation courses (adjusted odds ratio, 1.44; 95% CI, 1.04-2.01). The number of ventilation courses was not associated with increased risk of supplemental oxygen use at discharge after adjustment for the length of ventilation. A greater number of ventilation courses did not increase the risk of tracheostomy.
Conclusions and relevance: Among ELBW infants, a longer cumulative duration of mechanical ventilation largely accounts for the increased risk of chronic respiratory morbidity associated with reinitiation of mechanical ventilation. These results support attempts of extubation in ELBW infants receiving mechanical ventilation on low ventilator settings, even when success is not guaranteed.
Conflict of interest statement
Figures
References
-
- Sant’Anna GM, Keszler M. Weaning infants from mechanical ventilation. Clin Perinatol 2012;39(3): 543–562. - PubMed
-
- Ehrenkranz RA, Walsh MC, Vohr BR, et al. ; National Institutes of Child Health and Human Development Neonatal Research Network. Validation of the National Institutes of Health consensus definition of bronchopulmonary dysplasia. Pediatrics. 2005;116(6):1353–1360. - PubMed
-
- Walsh MC, Morris BH, Wrage LA, et al. ; National Institutes of Child Health and Human Development Neonatal Research Network. Extremely low birthweight neonates with protracted ventilation: mortality and 18-month neurodevelopmental outcomes. J Pediatr 2005;146(6):798–804. - PubMed
-
- Schmidt B, Roberts RS, Davis P, et al. ; Caffeine for Apnea of Prematurity Trial Group. Long-term effects of caffeine therapy for apnea of prematurity. N Engl J Med 2007;357(19):1893–1902. - PubMed
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
