

Prospective Study on Noninvasive Assessment of Intracranial Pressure in Traumatic Brain-Injured Patients: Comparison of Four Methods
- PMID: 26414916
- PMCID: PMC4841086
- DOI: 10.1089/neu.2015.4134
Prospective Study on Noninvasive Assessment of Intracranial Pressure in Traumatic Brain-Injured Patients: Comparison of Four Methods
Abstract
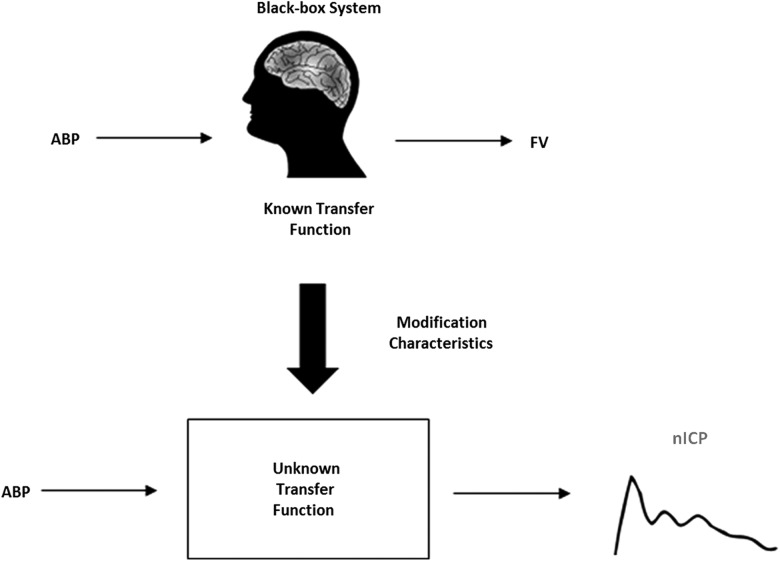
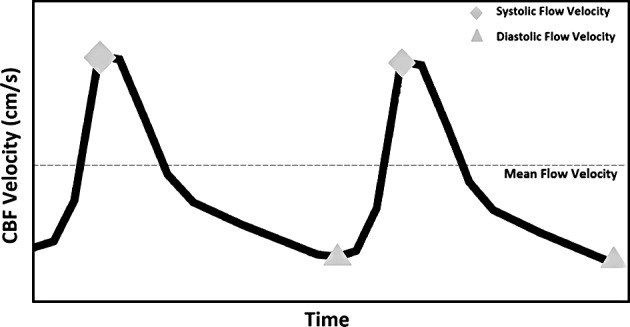
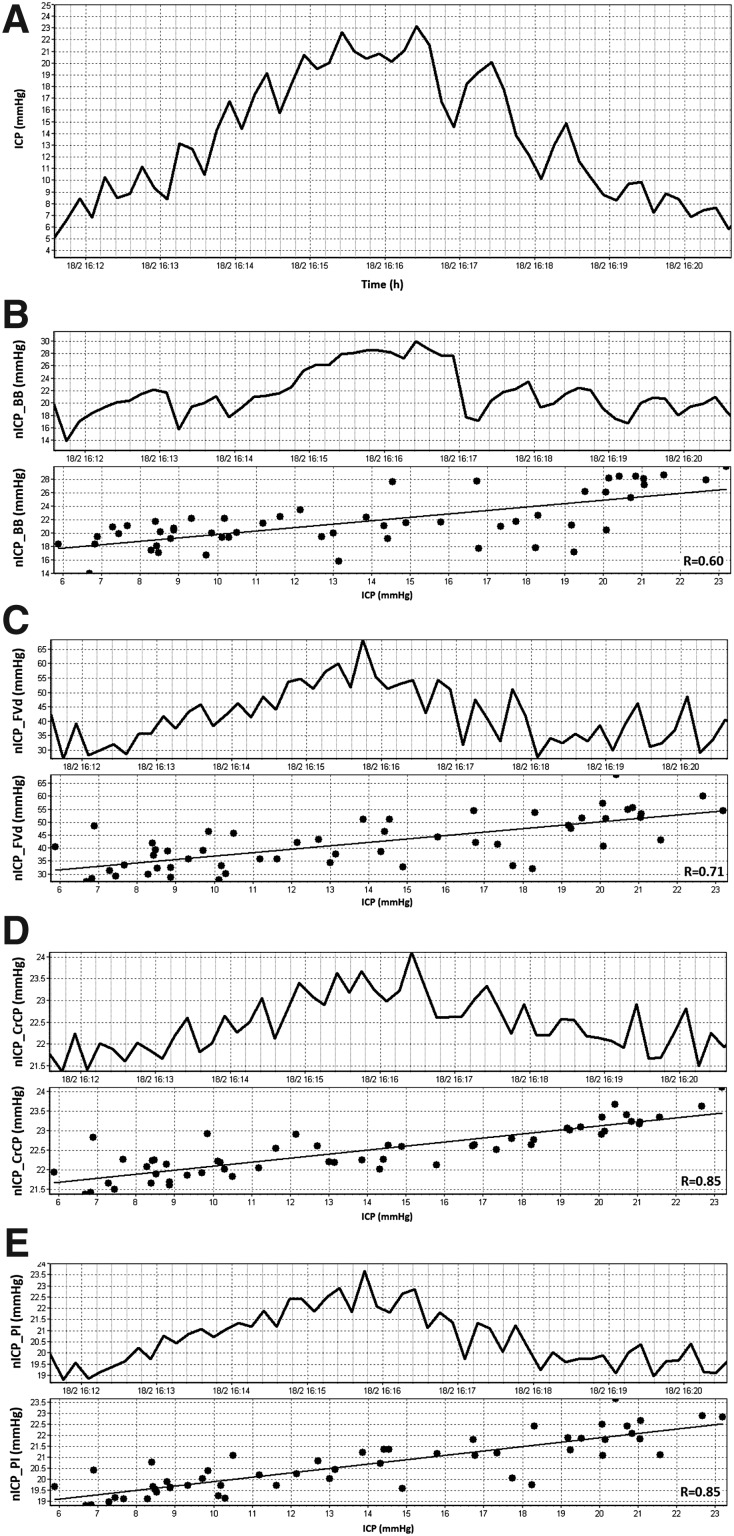
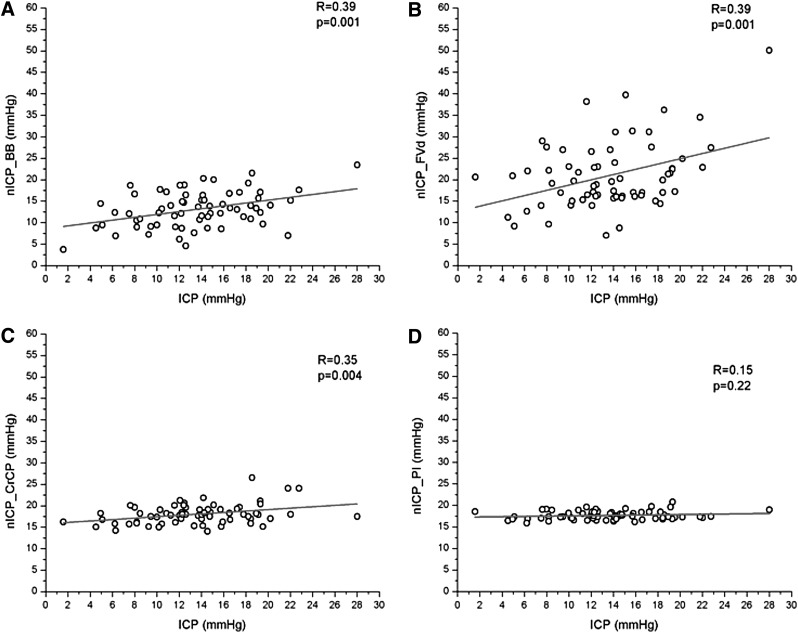
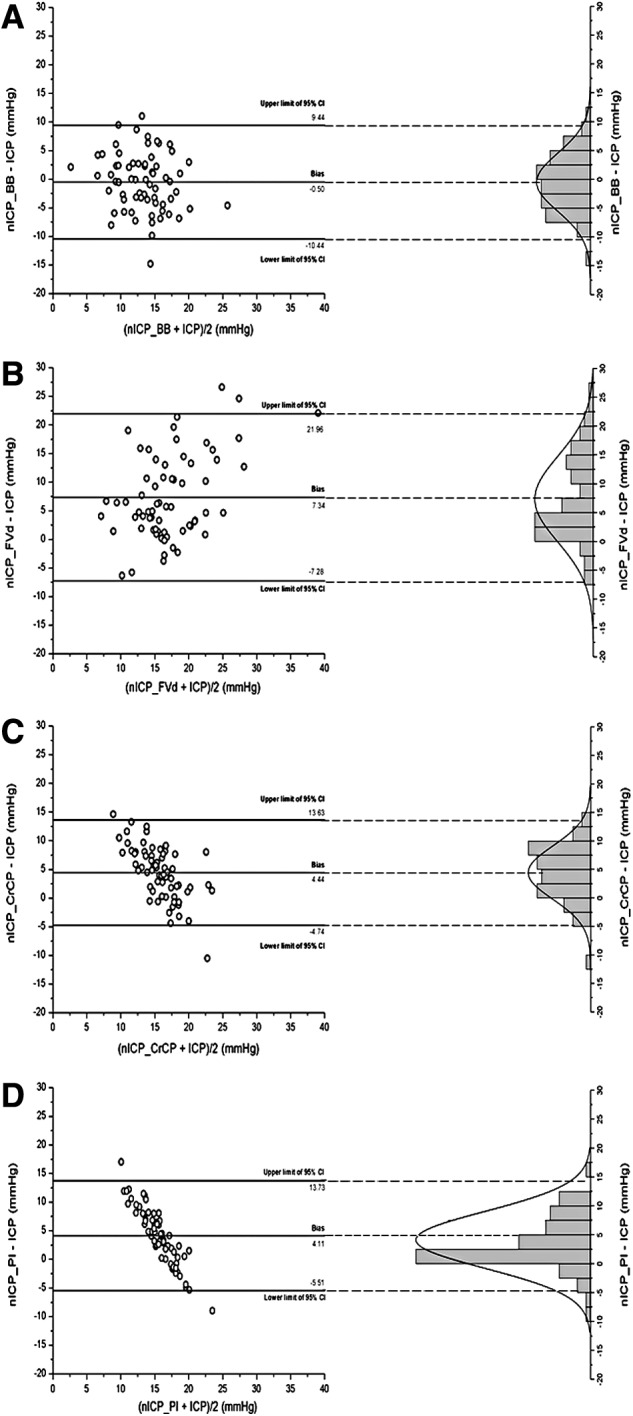
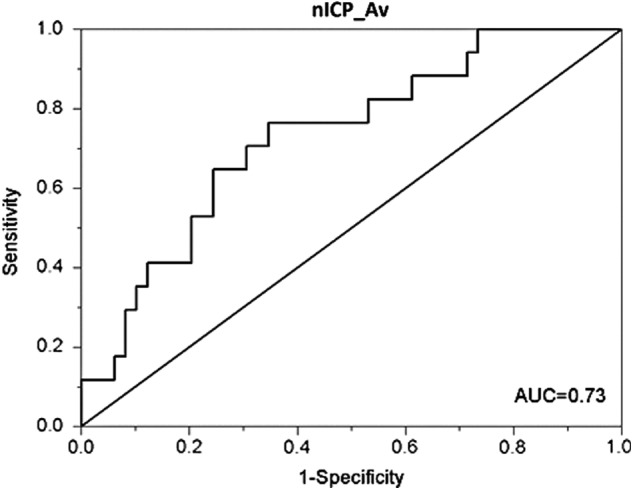
Elevation of intracranial pressure (ICP) may occur in many diseases, and therefore the ability to measure it noninvasively would be useful. Flow velocity signals from transcranial Doppler (TCD) have been used to estimate ICP; however, the relative accuracy of these methods is unclear. This study aimed to compare four previously described TCD-based methods with directly measured ICP in a prospective cohort of traumatic brain-injured patients. Noninvasive ICP (nICP) was obtained using the following methods: 1) a mathematical "black-box" model based on interaction between TCD and arterial blood pressure (nICP_BB); 2) based on diastolic flow velocity (nICP_FVd); 3) based on critical closing pressure (nICP_CrCP); and 4) based on TCD-derived pulsatility index (nICP_PI). In time domain, for recordings including spontaneous changes in ICP greater than 7 mm Hg, nICP_PI showed the best correlation with measured ICP (R = 0.61). Considering every TCD recording as an independent event, nICP_BB generally showed to be the best estimator of measured ICP (R = 0.39; p < 0.05; 95% confidence interval [CI] = 9.94 mm Hg; area under the curve [AUC] = 0.66; p < 0.05). For nICP_FVd, although it presented similar correlation coefficient to nICP_BB and marginally better AUC (0.70; p < 0.05), it demonstrated a greater 95% CI for prediction of ICP (14.62 mm Hg). nICP_CrCP presented a moderate correlation coefficient (R = 0.35; p < 0.05) and similar 95% CI to nICP_BB (9.19 mm Hg), but failed to distinguish between normal and raised ICP (AUC = 0.64; p > 0.05). nICP_PI was not related to measured ICP using any of the above statistical indicators. We also introduced a new estimator (nICP_Av) based on the average of three methods (nICP_BB, nICP_FVd, and nICP_CrCP), which overall presented improved statistical indicators (R = 0.47; p < 0.05; 95% CI = 9.17 mm Hg; AUC = 0.73; p < 0.05). nICP_PI appeared to reflect changes in ICP in time most accurately. nICP_BB was the best estimator for ICP "as a number." nICP_Av demonstrated to improve the accuracy of measured ICP estimation.
Keywords: noninvasive ICP monitoring; transcranial Doppler; traumatic brain injury.
Figures
References
-
- Hanlo P.W., Peters R.J.A., Gooskens R.H.J.M., Heethaar R.M., Keunen R.W.M., Van Huffelen A.C., Tulleken C.A.F., and Willemse J. (1995). Monitoring intracranial dynamics by transcranial Doppler—a new Doppler index: trans systolic time. Ultrasound Med. Biol. 21, 613–621 - PubMed
-
- Ueno T., Ballard R.E., Shuer L.M., Cantrell J.H., Yost W.T., and Hargens A.R. (1998). Noninvasive measurement of pulsatile intracranial pressure using ultrasound. Acta Neurochir. Suppl. 71, 66–69 - PubMed
-
- Michaeli D., and Rappaport Z.H. (2002). Tissue resonance analysis; a novel method for noninvasive monitoring of intracranial pressure. Technical note. J. Neurosurg. 96, 1132–1137 - PubMed
-
- Ragauskas A., Daubaris G., Ragaisis V., and Petkus V. (2003). Implementation of non-invasive brain physiological monitoring concepts. Med. Eng. Phys. 25, 667–678 - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
