

Cancer stem cells are the cause of drug resistance in multiple myeloma: fact or fiction?
- PMID: 26415231
- PMCID: PMC4747348
- DOI: 10.18632/oncotarget.5800
Cancer stem cells are the cause of drug resistance in multiple myeloma: fact or fiction?
Abstract
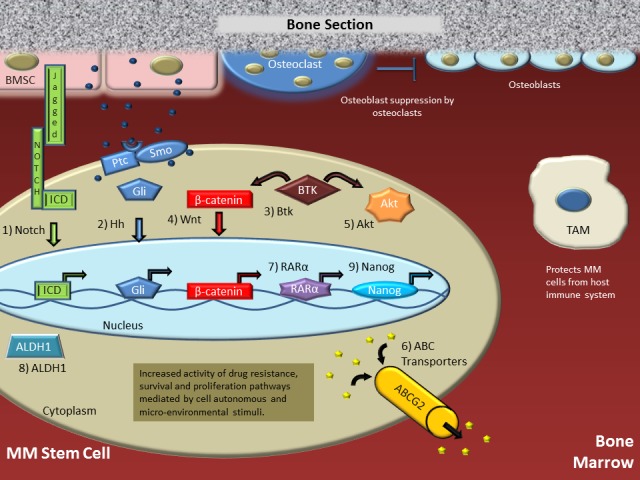
Multiple myeloma (MM) remains a largely incurable, genetically heterogeneous plasma-cell malignancy that contains - just like many other cancers - a small fraction of clonogenic stem cell-like cells that exhibit pronounced self-renewal and differentiation capacities, but also pronounced drug resistance. These MM stem cells (MMSCs) are a controversial but highly significant issue in myeloma research because, in our opinion, they are at the root of the failure of anti-neoplastic chemotherapies to transform myeloma to a manageable chronic disease. Several markers including CD138-, ALDH1+ and SP have been used to identify MMSCs; however, no single marker is reliable for the isolation of MMSC. Nonetheless, it is now known that MMSCs depend on self-renewal and pro-survival pathways, such as AKT, Wnt/β-catenin, Notch and Hedgehog, which can be targeted with novel drugs that have shown promise in pre-clinical and clinical trials. Here, we review the pathways of myeloma "stemness", the interactions with the bone marrow microenvironment that promote drug resistance, and the obstacles that must be overcome to eradicate MMSCs and make myeloma a curable disease.
Keywords: drug resistance; myeloma and other plasma cell dyscrasias; neoplasia; signaling therapies.
Conflict of interest statement
No potential conflicts of interest were disclosed.
Figures
References
-
- Palumbo A, K A. Multiple Myeloma. New England Journal of Medicine. 2011;364:1046–1060. - PubMed
-
- Hideshima T, Mitsiades C, Tonon G, Richardson PG, Anderson KC. Understanding multiple myeloma pathogenesis in the bone marrow to identify new therapeutic targets. Nat Rev Cancer. 2007;7:585–598. - PubMed
-
- Chesi M, Bergsagel P, Brents L, Smith C, Gerhard D, Kuehl W. Dysregulation of cyclin D1 by translocation into an IgH gamma switch region in two multiple myeloma cell lines. 1996;88:674–681. - PubMed
-
- Fonseca R, Barlogie B, Bataille R, Bastard C, Bergsagel PL, Chesi M, Davies FE, Drach J, Greipp PR, Kirsch IR, Kuehl WM, Hernandez JM, Minvielle S, et al. Genetics and Cytogenetics of Multiple Myeloma: A Workshop Report. Cancer Research. 2004;64:1546–1558. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
