

Lymphomatosis cerebri: a rare form of primary central nervous system lymphoma. Analysis of 7 cases and systematic review of the literature
- PMID: 26415875
- PMCID: PMC4827036
- DOI: 10.1093/neuonc/nov197
Lymphomatosis cerebri: a rare form of primary central nervous system lymphoma. Analysis of 7 cases and systematic review of the literature
Abstract
Background: Primary central nervous system lymphomas may present as diffuse, nonenhancing infiltrative lesions. This rare variant is termed lymphomatosis cerebri (LC). We did a systematic review and analysis of the literature, adding our own cases, to better characterize LC in order to improve early diagnosis and treatment.
Methods: PubMed, ISI Web of Knowledge, and hospital databases were reviewed. Information was extracted regarding demographic, clinical, histological, cerebrospinal fluid (CSF), neuroimaging, and treatment variables. The impact of single parameters on overall survival (OS) was determined by applying univariate and multivariate analyses.
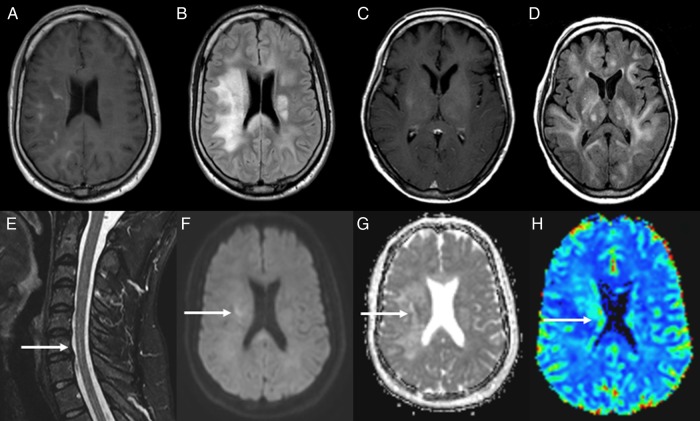
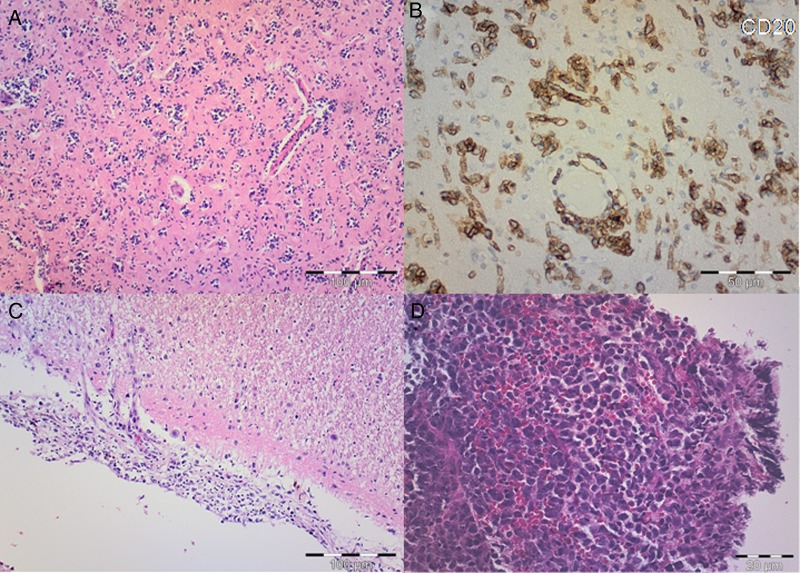
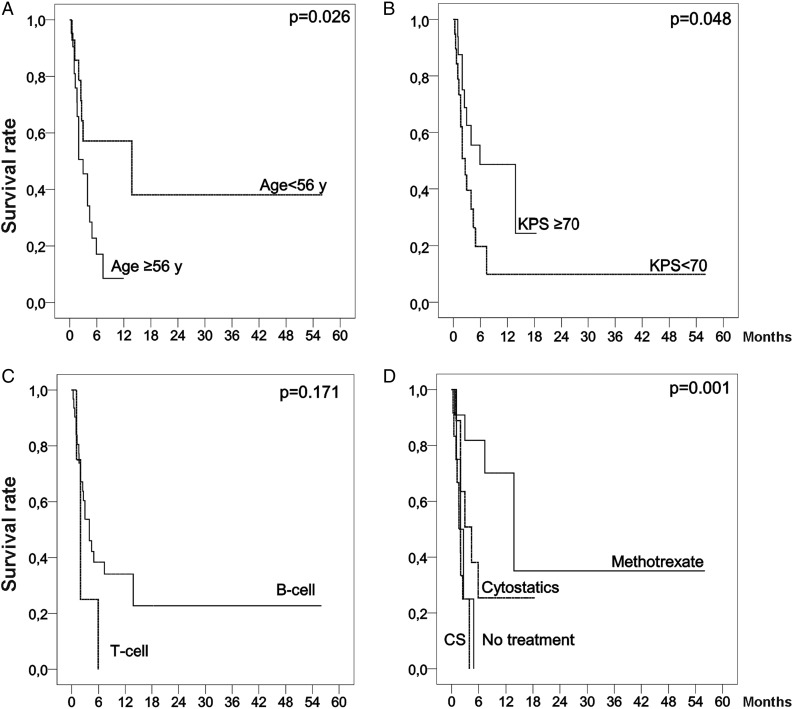
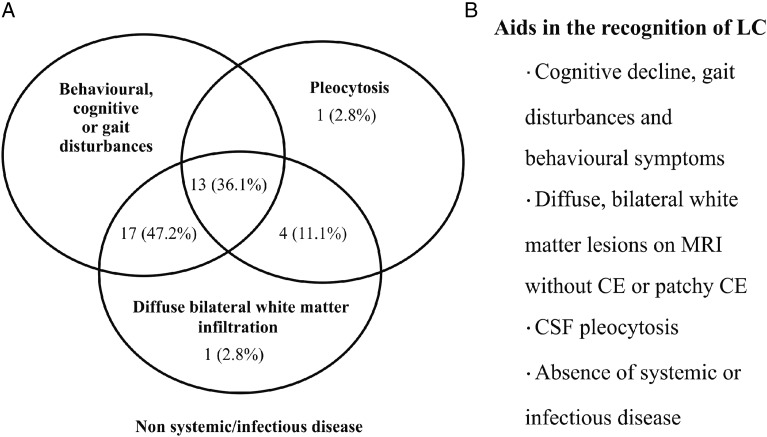
Results: Forty-two patients were included (median age: 58 y; range: 28-80 y). At consultation, 52% of patients had a poor KPS. The most common presenting symptom was cognitive decline (59.5%). Imaging studies showed supratentorial and infratentorial infiltration in 55% of patients and bilateral hemispheric involvement in 95%. CSF pleocytosis was present in 51.5% of the patients. Median time to diagnosis was 4.5 (range: 1-30) months, and the diagnosis was not established until autopsy for 33% of patients. The median OS was 2.95 (range: 0.33-56) months; however, those patients who received methotrexate had a median OS of 13.8 (range: 0.7-56) months. Analysis identified KPS ≥ 70 (HR: 0.32; 95% CI: 0.114-0.894; P = .03) and treatment with methotrexate (HR: 0.19; 95% CI: 0.041-0.886; P = .034) as independent favorable prognostic factors, whereas T-cell lymphoma was independently related with a worse outcome (HR: 6.62; 95% CI: 1.317-33.316; P = .022).
Conclusions: LC is a misdiagnosed entity associated with considerable diagnostic delay. MRI evidence of bilateral hemispheric involvement and CSF pleocytosis should be alerts for this diagnosis. Treatment with methotrexate-based chemotherapy must be considered, especially for patients with good KPS.
Keywords: diffuse infiltrative lesion; leukoencephalopathy; lymphomatosis cerebri; primary central nervous system lymphoma.
© The Author(s) 2015. Published by Oxford University Press on behalf of the Society for Neuro-Oncology. All rights reserved. For permissions, please e-mail: journals.permissions@oup.com.
Figures
References
-
- Hong JT, Chae JB, Lee JY, Kim JG, Yoon YH. Ocular involvement in patients with primary CNS lymphoma. J Neurooncol. 2011;102(1):139–145. - PubMed
-
- Kuker W, Nagele T, Thiel E, Weller M, Herrlinger U. Primary central nervous system lymphomas (PCNSL): MRI response criteria revised. Neurology. 2005;65(7):1129–1131. - PubMed
-
- Ferreri AJ, Marturano E. Primary CNS lymphoma. Best Pract Res Clin Haematol. 2012;25(1):119–130. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
