

The negative impact of spasticity on the health-related quality of life of stroke survivors: a longitudinal cohort study
- PMID: 26415945
- PMCID: PMC4587810
- DOI: 10.1186/s12955-015-0340-3
The negative impact of spasticity on the health-related quality of life of stroke survivors: a longitudinal cohort study
Abstract
Background: Spasticity often leads to symptomatic and functional problems that can cause disability for stroke survivors. We studied whether spasticity has a negative impact on health-related quality of life (HRQoL).
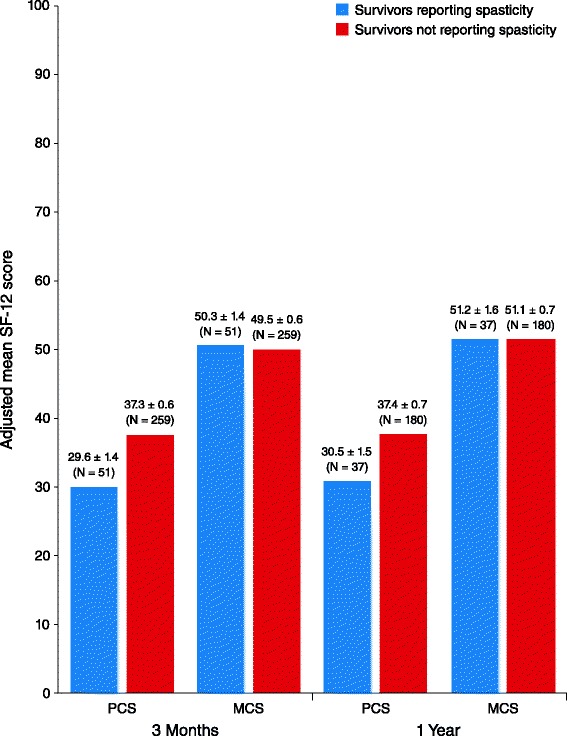
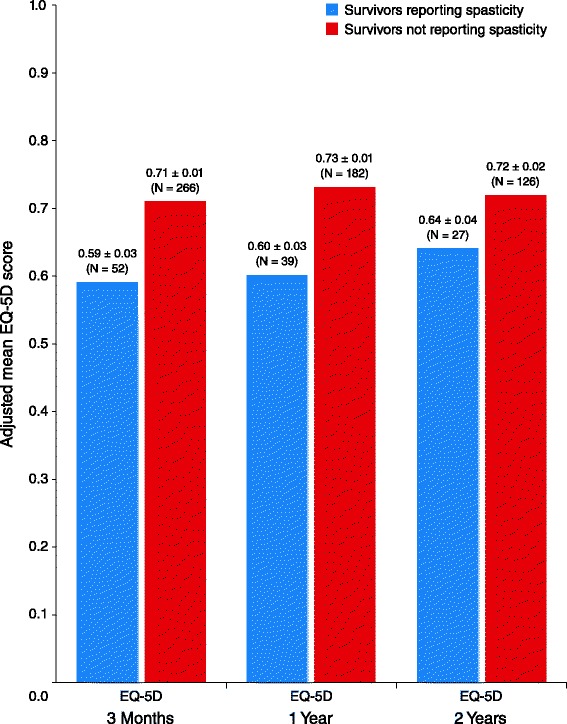
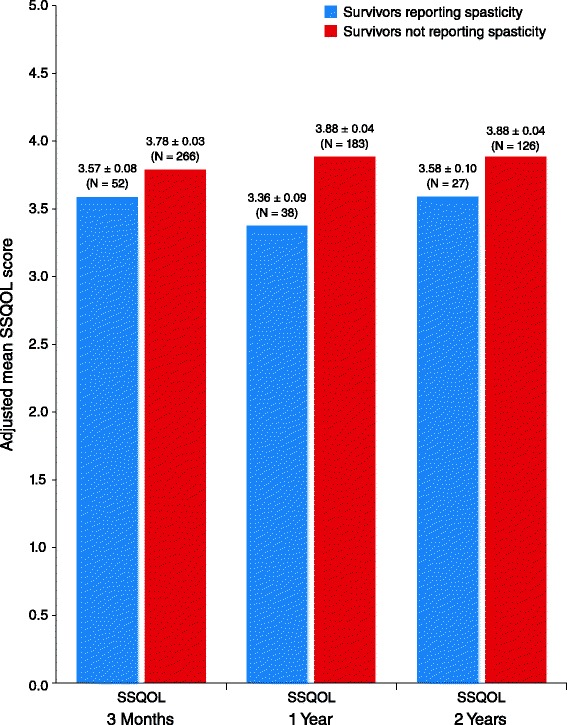
Methods: As part of the Greater Cincinnati/Northern Kentucky Stroke Study (NCT00642213), 460 ischemic stroke patients were interviewed during hospitalization and then followed over time. HRQoL was measured by the Physical Component Summary (PCS) and Mental Component Summary (MCS) scores of the Short Form-12 (SF-12), EuroQol-5 dimension (EQ-5D), and Stroke-Specific Quality of Life (SSQOL) instruments, with lower scores indicating worse health. HRQoL differences between stroke survivors with and without spasticity were compared, adjusting for age, race, stroke severity, pre-stroke function, and comorbidities.
Results: Of the 460 ischemic stroke patients, 328 had spasticity data available 3 months after their stroke (mean age of 66 years, 49% were female, and 26% were black). Of these patients, 54 (16%) reported having spasticity. Three months following their stroke, patients who reported spasticity had lower mean scores on the PCS (29.6 ± 1.4 vs 37.3 ± 0.6; P < .001), EQ-5D (0.59 ± 0.03 vs 0.71 ± 0.01; P < .001), and SSQOL (3.57 ± 0.08 versus 3.78 ± 0.03; P = .03) compared with patients who did not report spasticity. Lower HRQoL scores were also observed at the 1-year (PCS, EQ-5D, and SSQOL) and 2-year (EQ-5D and SSQOL) interviews in those with spasticity compared with those without spasticity.
Conclusions: Statistically and clinically meaningful differences in HRQoL exist between stroke survivors with and without spasticity.
Figures
References
-
- Mackay J, Mensah G. The atlas of heart disease and stroke. Geneva: World Health Organization; 2004.
Publication types
MeSH terms
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
