

Robotic Approaches to Palatoplasty and the Treatment of Velopharyngeal Dysfunction
- PMID: 26417207
- PMCID: PMC4572729
- DOI: 10.1055/s-0034-1368165
Robotic Approaches to Palatoplasty and the Treatment of Velopharyngeal Dysfunction
Abstract
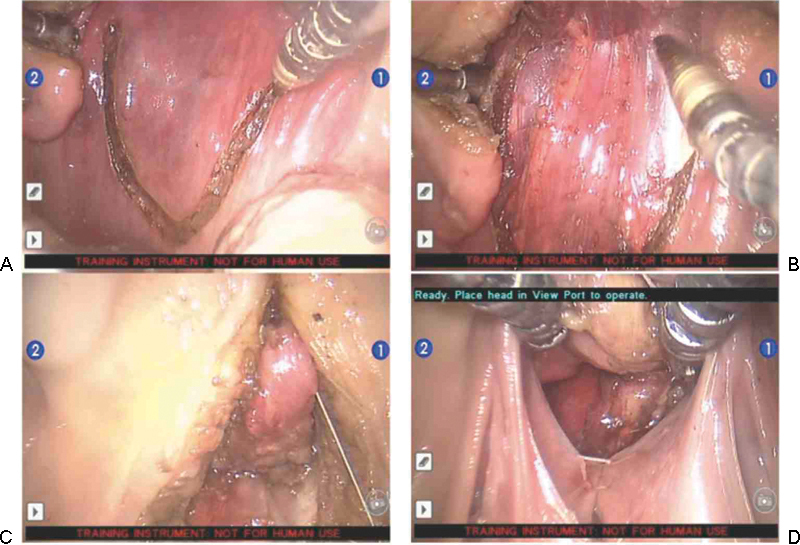
The operative techniques used to address palatoplasty and velopharyngeal dysfunction rely on traditional methods of surgical exposure and tissue handling. As the role of robotic surgical systems has expanded, emphasis has shifted from extirpative to reconstructive applications. We discuss the possible role of surgical telemanipulation systems in the treatment of these diagnoses. Furthermore, we present a feasibility study that addresses a commonly performed treatment of velopharyngeal dysfunction-posterior pharyngeal flap (PPF). In brief, PPFs were successfully performed on a small series of cadaveric human specimens. The technical aspects of the procedure, including telemanipulator set-up, positioning, surgical instrumentation, and timing are described in detail. All cadavers underwent successful performance of PPFs. Operative times were within an acceptable range and use of the robotic system demonstrated a steep learning curve. Many of the potential advantages and costs associated with robotic surgical systems are discussed.
Keywords: palatoplasty; robotic surgery; velopharyngeal dysfunction.
Figures
References
-
- Liau J Y, Sadove A M, van Aalst J A. An evidence-based approach to cleft palate repair. Plast Reconstr Surg. 2010;126(6):2216–2221. - PubMed
-
- Katz R D, Taylor J A, Rosson G D, Brown P R, Singh N K. Robotics in plastic and reconstructive surgery: use of a telemanipulator slave robot to perform microvascular anastomoses. J Reconstr Microsurg. 2006;22(1):53–57. - PubMed
-
- Katz R D, Rosson G D, Taylor J A, Singh N K. Robotics in microsurgery: use of a surgical robot to perform a free flap in a pig. Microsurgery. 2005;25(7):566–569. - PubMed
-
- Smartt J M Jr, Singh D J, Reid R R, Hellinger J C, Hsu V M, Bartlett S P. Squamosal suture synostosis: a cause of atypical skull asymmetry. Plast Reconstr Surg. 2012;130(1):165–176. - PubMed
-
- Mirzabeigi M N, Lee M, Smartt J M Jr, Jandali S, Sonnad S S, Serletti J M. Extended trimethoprim/sulfamethoxazole prophylaxis for implant reconstruction in the previously irradiated chest wall. Plast Reconstr Surg. 2012;129(1):37e–45e. - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials
