

The role of healthcare providers in the roll out of preexposure prophylaxis
- PMID: 26417953
- PMCID: PMC4676563
- DOI: 10.1097/COH.0000000000000206
The role of healthcare providers in the roll out of preexposure prophylaxis
Abstract
Purpose of review: To review the most recent studies assessing the preparedness of healthcare practitioners to provide anti-HIV preexposure prophylaxis (PrEP) and suggest areas for future implementation research.
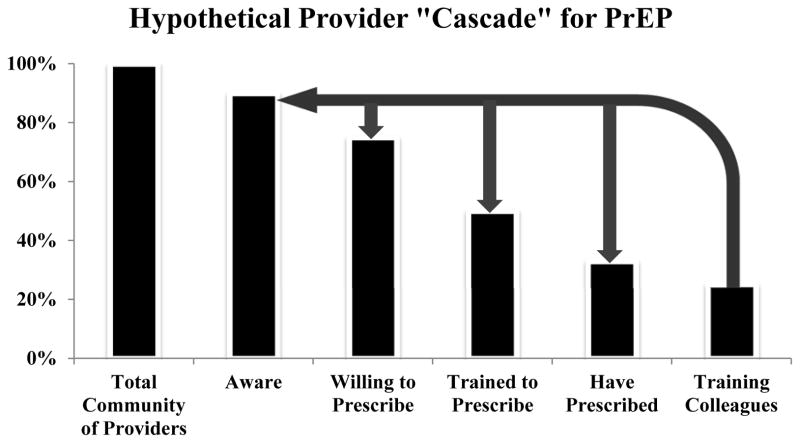
Recent findings: As PrEP is a biobehavioral intervention, healthcare providers are likely to play a critical role in implementing PrEP in care settings. Studies suggest that many specialized providers are aware of PrEP and support its provision as a public health intervention, though knowledge and acceptance are less among generalists. Therefore, utilization of PrEP by clinicians has been limited to a few early adopters. Concerns about the efficacy and long-term safety of PrEP, and perceived barriers to prescribing PrEP, could limit prescribing behaviors and intentions. Resistance to performing routine HIV risk assessments by clinicians is an additional barrier to implementing PrEP, although innovative tools to help clinicians routinely perform risk assessments, are being developed.
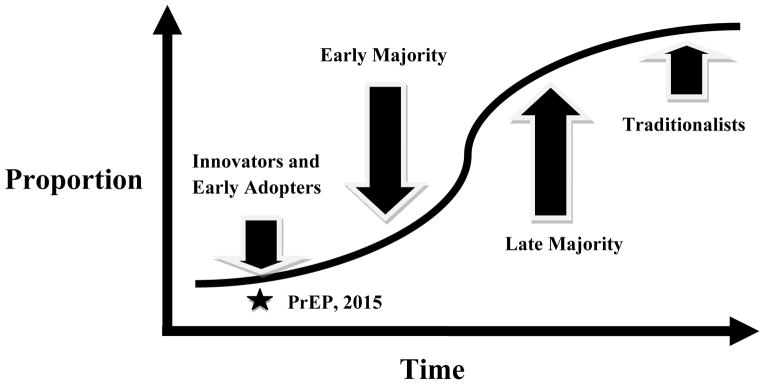
Summary: Interventions are needed to engage a broader array of healthcare providers in PrEP provision. Utilizing a framework based on diffusion of innovation theory, this review proposes strategies that can be implemented and evaluated to increase PrEP prescribing by healthcare providers. If resources are invested in training clinicians to provide PrEP, then these stakeholders could enhance the use of PrEP as part of a prevention package by primary providers.
Conflict of interest statement
K.H.M. has conducted research with unrestricted project support from Gilead Sciences and Merck. D.S. K. has conducted research with unrestricted project support from Gilead Sciences and Bristol Myers Squibb.
Figures
References
-
- Choopanya K, Martin M, Suntharasamai P, Sangkum U, Mock PA, Leethochawalit M, et al. Antiretroviral prophylaxis for HIV infection in injecting drug users in Bangkok, Thailand (the Bangkok Tenofovir Study): a randomised, double-blind, placebo-controlled phase 3 trial. Lancet. 2013 Jun 15;381(9883):2083–90. - PubMed
-
- Marrazzo JM, Ramjee G, Richardson BA, Gomez K, Mgodi N, Nair G, et al. Tenofovir-based preexposure prophylaxis for HIV infection among African women. N Engl J Med. 2015 Feb 5;372(6):509–18. This study was unable to demonstrate the efficacy of oral and topical pre-exposure prophylaxis with tenofovir-based regimens among young women in sub-Saharan Africa, likely due to low adherence among study participants. - PMC - PubMed
-
- Thigpen MC, Kebaabetswe PM, Paxton LA, Smith DK, Rose CE, Segolodi TM, et al. Antiretroviral preexposure prophylaxis for heterosexual HIV transmission in Botswana. N Engl J Med. 2012 Aug 2;367(5):423–34. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
