

Progression of Liver Fibrosis in HIV/HCV Co-Infection: A Comparison between Non-Invasive Assessment Methods and Liver Biopsy
- PMID: 26418061
- PMCID: PMC4587859
- DOI: 10.1371/journal.pone.0138838
Progression of Liver Fibrosis in HIV/HCV Co-Infection: A Comparison between Non-Invasive Assessment Methods and Liver Biopsy
Abstract
Objectives: To evaluate the diagnostic performance of seven non-invasive tests (NITs) of liver fibrosis and to assess fibrosis progression over time in HIV/HCV co-infected patients.
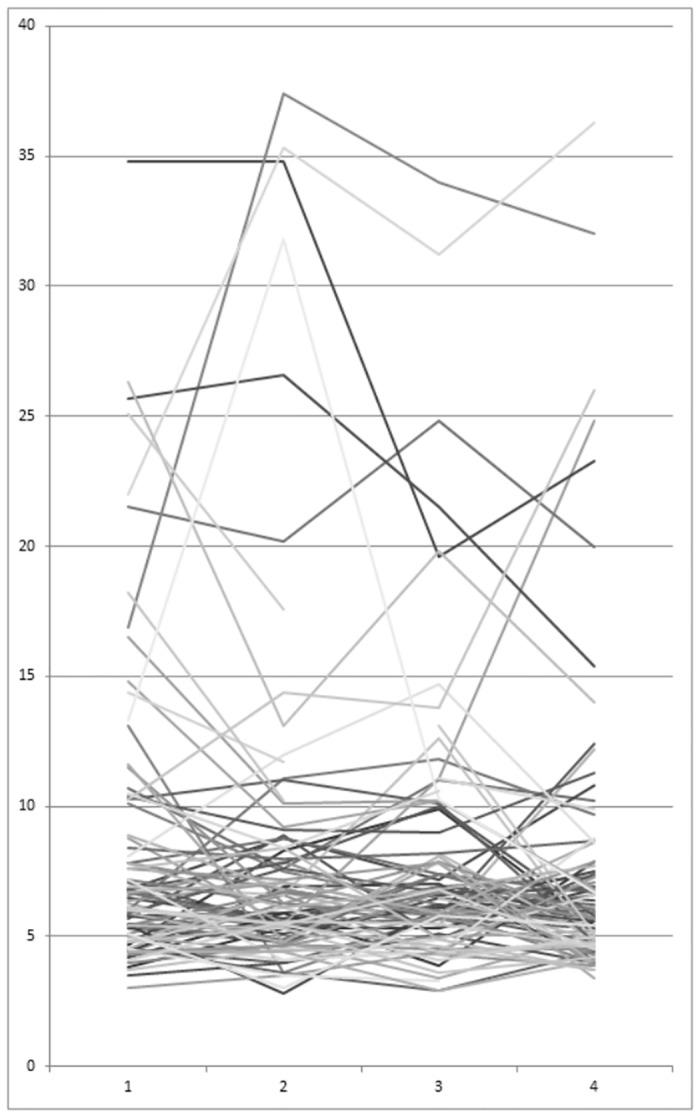
Methods: Transient elastography (TE) and six blood tests were compared to histopathological fibrosis stage (METAVIR). Participants were followed over three years with NITs at yearly intervals.
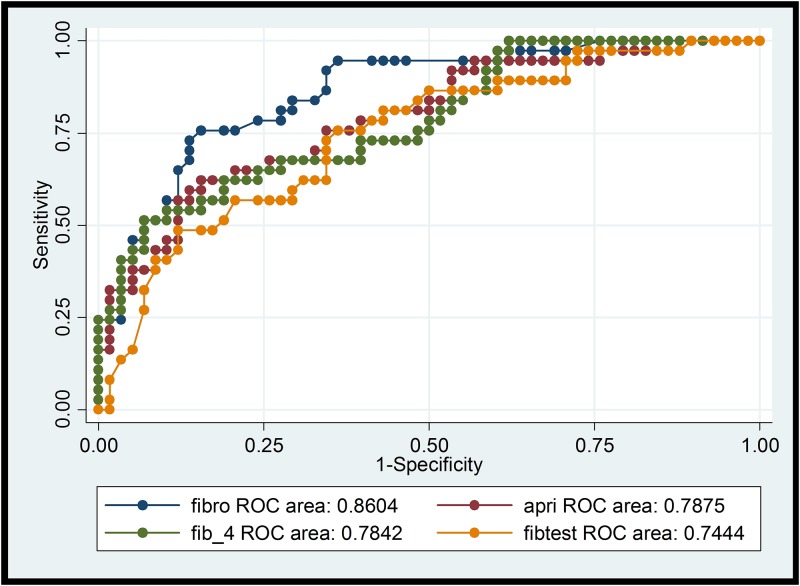
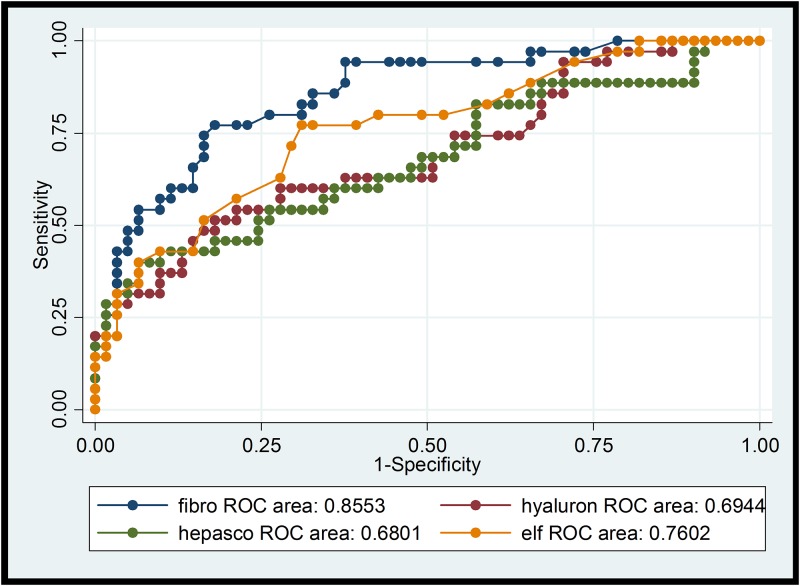
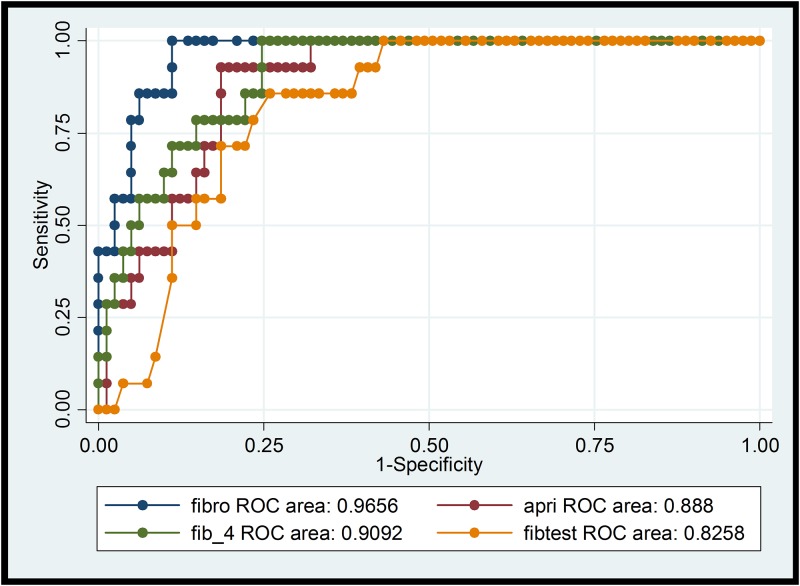
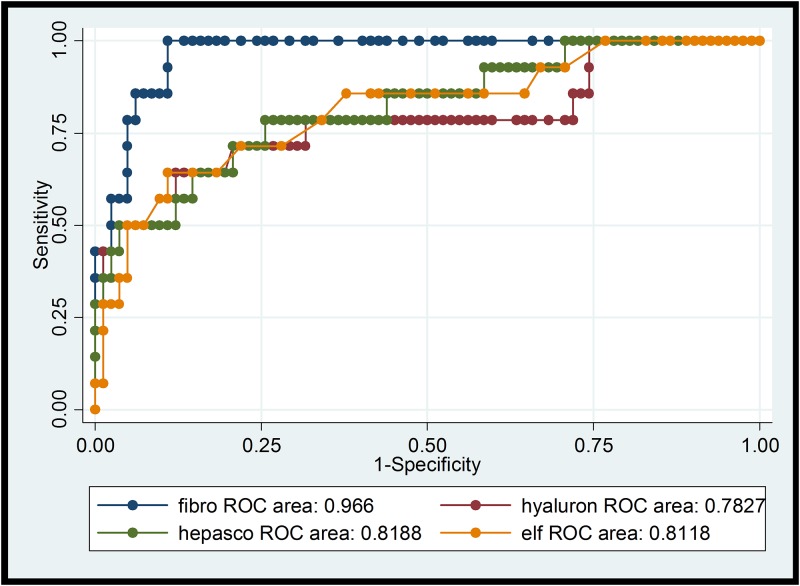
Results: Area under the receiver operating characteristic curve (AUROC) for significant fibrosis (> = F2) in 105 participants was highest for TE (0.85), followed by FIB-4 (0.77), ELF-Test (0.77), APRI (0.76), Fibrotest (0.75), hyaluronic acid (0.70), and Hepascore (0.68). AUROC for cirrhosis (F4) was 0.97 for TE followed by FIB-4 (0.91), APRI (0.89), Fibrotest (0.84), Hepascore (0.82), ELF-Test (0.82), and hyaluronic acid (0.79). A three year follow-up was completed by 87 participants, all on antiretroviral therapy and in 20 patients who completed HCV treatment (9 with sustained virologic response). TE, APRI and Fibrotest did not significantly change during follow-up. There was weak evidence for an increase of FIB-4 (mean increase: 0.22, p = 0.07). 42 participants had a second liver biopsy: Among 38 participants with F0-F3 at baseline, 10 were progessors (1-stage increase in fibrosis, 8 participants; 2-stage, 1; 3-stage, 1). Among progressors, mean increase in TE was 3.35 kPa, in APRI 0.36, and in FIB-4 0.75. Fibrotest results did not change over 3 years.
Conclusion: TE was the best NIT for liver fibrosis staging in HIV/HCV co-infected patients. APRI-Score, FIB-4 Index, Fibrotest, and ELF-Test were less reliable. Routinely available APRI and FIB-4 performed as good as more expensive tests. NITs did not change significantly during a follow-up of three years, suggesting slow liver disease progression in a majority of HIV/HCV co-infected persons on antiretroviral therapy.
Conflict of interest statement
Figures
References
-
- Macías J, Márquez M, Téllez F, Merino D, Jiménez-Aguilar P, López-Cortés LF, et al. Risk of liver decompensation among HIV/hepatitis C virus-coinfected individuals with advanced fibrosis: implications for the timing of therapy. Clin Infect Dis Off Publ Infect Dis Soc Am. 2013;57: 1401–1408. 10.1093/cid/cit537 - DOI - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
