

Tylosis with oesophageal cancer: Diagnosis, management and molecular mechanisms
- PMID: 26419362
- PMCID: PMC4589029
- DOI: 10.1186/s13023-015-0346-2
Tylosis with oesophageal cancer: Diagnosis, management and molecular mechanisms
Abstract
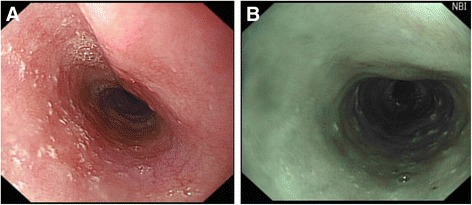
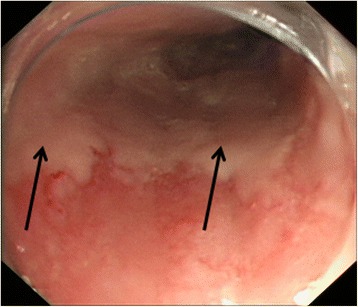
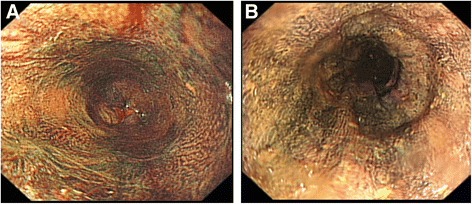
Tylosis (hyperkeratosis palmaris et plantaris) is characterised by focal thickening of the skin of the hands and feet and is associated with a very high lifetime risk of developing squamous cell carcinoma of the oesophagus. This risk has been calculated to be 95% at the age of 65 in one large family, however the frequency of the disorder in the general population is not known and is likely to be less than one in 1,000,000. Oesophageal lesions appear as small (2-5 mm), white, polyploid lesions dotted throughout the oesophagus and oral leukokeratosis has also been described. Although symptoms of oesophageal cancer can include dysphagia, odynophagia, anorexia and weight loss, there may be an absence of symptoms in early disease, highlighting the importance of endoscopic surveillance in these patients. Oesophageal cancer associated with tylosis usually presents in middle to late life (from mid-fifties onwards) and shows no earlier development than the sporadic form of the disease. Tylosis with oesophageal cancer is inherited as an autosomal dominant trait with complete penetrance of the cutaneous features, usually by 7 to 8 years of age but can present as late as puberty. Mutations in RHBDF2 located on 17q25.1 have recently been found to be causative. A diagnosis of tylosis with oesophageal cancer is made on the basis of a positive family history, characteristic clinical features, including cutaneous and oesophageal lesions, and genetic analysis for mutations in RHBDF2. The key management goal is surveillance for early detection and treatment of oesophageal dysplasia. Surveillance includes annual gastroscopy with biopsy of any suspicious lesion together with quadratic biopsies from the upper, middle and lower oesophagus. This is coupled with dietary and lifestyle modification advice and symptom education. Symptomatic management of the palmoplantar keratoderma includes regular application of emollients, specialist footwear and early treatment of fissures and super-added infection, particularly tinea pedis. More specific treatment for the thick skin is available in the form of oral retinoids, which are very effective but commonly produce side effects, including nasal excoriation and bleeding, hypercholesterolaemia, and abnormal liver function tests. Genetic counselling can be offered to patients and family members once a family history has been established. The prognosis of tylosis with oesophageal cancer is difficult to determine due to the limited number of affected individuals. In the last 40 years of surveillance, five out of six cases of squamous oesophageal cancer in the Liverpool family were detected endoscopically and were surgically removed. Four of five patients had stage 1 disease at presentation and remain alive and well more than 8 years later. This suggests that the presence of a screening program improves prognosis for these patients.
Figures
References
-
- Howel-Evans W, McConnell RB, Clarke CA, Sheppard PM. Carcinoma of the oesophagus with keratosis palmaris et plantaris (Tylosis) Quart J Med. 1958;27:413–429. - PubMed
-
- Ellis A, Field JK, Field AE, Friedmann PS, Fryer A, Howard P, Leigh IM, Risk JM, Shaw JM, Whittaker J. Tylosis associated with carcinoma of the oesophagus and oral leukoplakia in a large Liverpool family—a review of six generations. Eur J Cancer B Oral Oncol. 1994;30B:102–112. doi: 10.1016/0964-1955(94)90061-2. - DOI - PubMed
-
- Harper PS, Harper RM, Howel-Evans AW. Carcinoma of the oesophagus with tylosis. Quart J Med. 1970;39:317–33. - PubMed
-
- Stevens HP, Kelsell DP, Bryant SP, Bishop DT, Spurr NK, Weissenbach J, Marger D, Marger RS, Leigh IM. Linkage of an American pedigree with palmoplantar keratoderma and malignancy(palmoplantar ectodermal dysplasia type III) to 17q24. Literature survey and proposed updated classification of the keratodermas. Arch. Dermatol. 1996;132:640–651. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
