

Heterogeneity of aquaporin-4 localization and expression after focal cerebral ischemia underlies differences in white versus grey matter swelling
- PMID: 26419740
- PMCID: PMC4588314
- DOI: 10.1186/s40478-015-0239-6
Heterogeneity of aquaporin-4 localization and expression after focal cerebral ischemia underlies differences in white versus grey matter swelling
Abstract
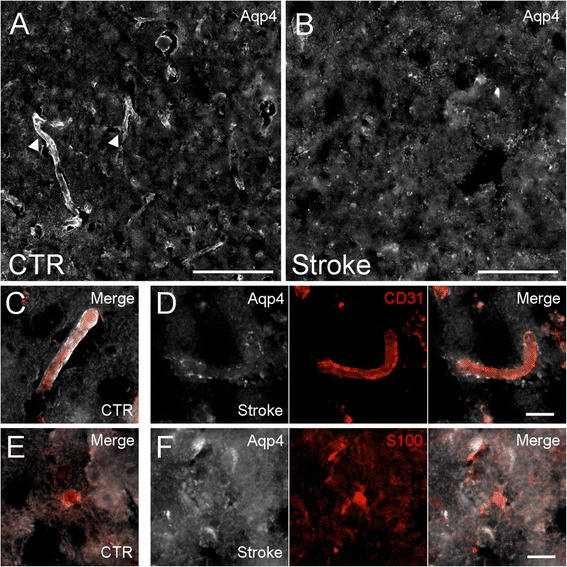
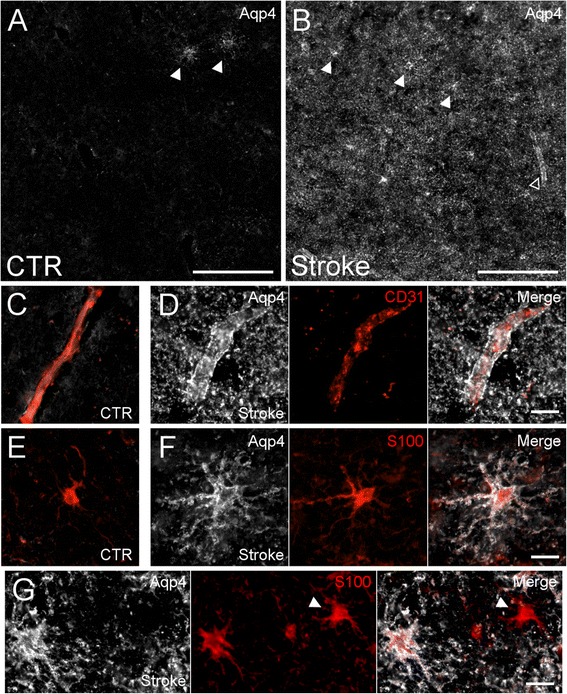
Introduction: Ischemic stroke, a major cause of mortality, is frequently accompanied by life-threatening cerebral edema. Aquaporin-4 (Aqp4), an astrocytic transmembrane water channel, is an important molecular contributor to cerebral edema formation. Past studies of Aqp4 expression and localization after ischemia examined grey matter exclusively. However, as white matter astrocytes differ developmentally, physiologically, and molecularly from grey matter astrocytes, we hypothesized that functionally important regional heterogeneity exists in Aqp4 expression and subcellular localization following cerebral ischemia.
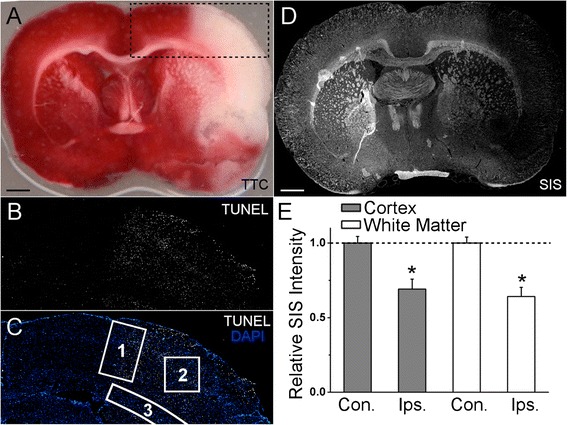
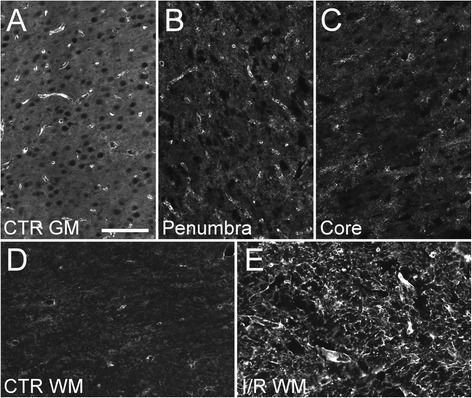
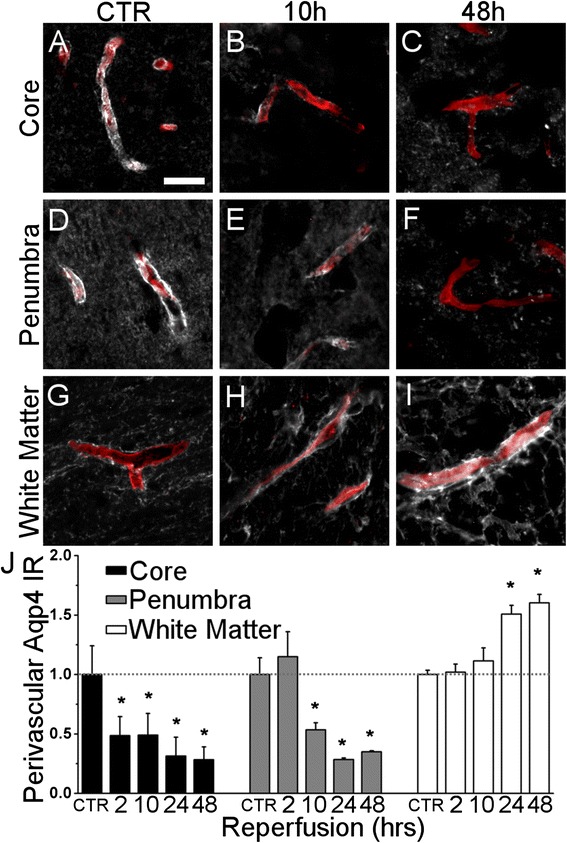
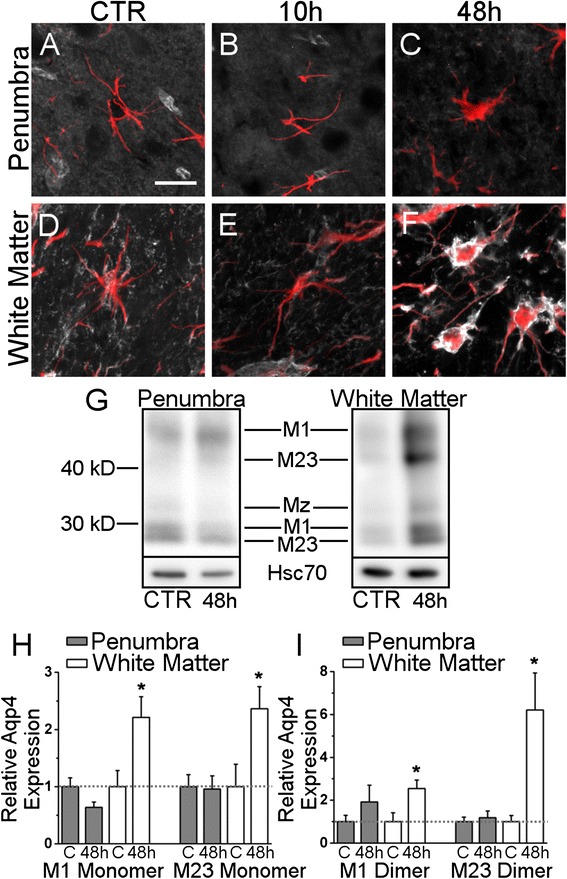
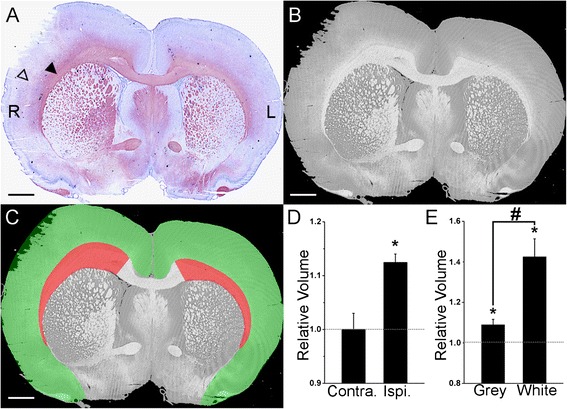
Results: Subcellular localization of Aqp4 was compared between cortical and white matter astrocytes in postmortem specimens of patients with focal ischemic stroke versus controls. Subcellular localization and expression of Aqp4 was examined in rats subjected to experimental stroke. Volumetric analysis was performed on the cortex and white matter of rats subjected to experimental stroke. Following cerebral ischemia, cortical astrocytes exhibited reduced perivascular Aqp4 and unchanged Aqp4 protein abundance. In contrast, white matter astrocytes exhibited increased perivascular and plasmalemmal Aqp4 and a 2.2- to 6.2-fold increase in Aqp4 isoform abundance. Ischemic white matter swelled by approximately 40 %, while cortex swelled by approximately 9 %.
Conclusions: The findings reported here raise the possibility that cerebral white matter may play a heretofore underappreciated role in the formation of cerebral edema following ischemia.
Figures
References
-
- Lozano R, Naghavi M, Foreman K, Lim S, Shibuya K, Aboyans V, et al. Global and regional mortality from 235 causes of death for 20 age groups in 1990 and 2010: a systematic analysis for the Global Burden of Disease Study 2010. Lancet. 2012;380:2095–128. doi: 10.1016/S0140-6736(12)61728-0. - DOI - PMC - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Miscellaneous
