

Adherence to Anti-tuberculosis treatment and treatment outcomes among tuberculosis patients in Alamata District, northeast Ethiopia
- PMID: 26420164
- PMCID: PMC4588463
- DOI: 10.1186/s13104-015-1452-x
Adherence to Anti-tuberculosis treatment and treatment outcomes among tuberculosis patients in Alamata District, northeast Ethiopia
Abstract
Background: Non-adherence to tuberculosis (TB) treatment can result in an emergence of new strains, prolonged infectiousness, drug resistance and poor treatment outcomes. Thus, assessment of the level of adherence to anti-TB treatment, treatment outcomes and identifying factors associated with non-adherence and poor treatment outcomes are vital for improving TB treatment adherence and treatment outcomes in the study area. The main objectives of the current study were to assess the level of adherence to anti-TB treatment among patients taking anti-TB drug treatment and to identify factors associated with non-adherence. Whereas, the secondary objectives were to assess treatment outcomes and factors associated with poor treatment outcomes among TB patients previously treated at the health institutions of Alamata District, northeast Ethiopia.
Methods: In a health facility-based cross-sectional study, TB patients who were taking anti-TB drug treatment were interviewed using a structured questionnaire to evaluate level of adherence to anti-TB treatment. TB treatment outcomes were evaluated using data generated from a record review of previous TB patients who were treated at health facilities of Alamata District from January 2007 to June 2012. Adherence data and treatment outcomes data were computerized separately using Epi-Data version 3.1 and analyzed using STATA version 10.0.
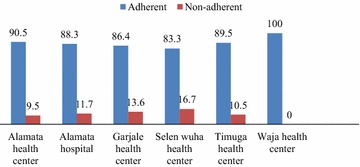
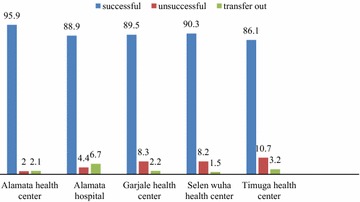
Results: Between November 2012 and January 2013, 116 (58.0%) male TB patients and 84 (42.0%) female TB patients were interviewed, of whom 77.5% were new cases, 23.5% were smear-positive pulmonary TB (SPPTB) cases, 26.5% were smear-negative PTB (SNPTB) cases and 50.0% were extra pulmonary (EPTB) cases. The overall adherence rate to anti-TB treatment was 88.5%. The main reasons for the non-adherent patients were forgetting to take medication, being away from home, drug side effects, being unable to go to the health facilities on the date of appointment and being hospitalized. In the TB treatment outcomes component of the current study, records of 4,275 TB patients were reviewed and the overall treatment success rate was 90.1%. Two-hundred fifteen (5.0%) patients had unsuccessful treatment outcomes, of whom 76 (35.3%) defaulted, 126 (58.6%) died and 13 (6.1%) had treatment failure. Significant predictors of unsuccessful treatment outcomes were being positive for human immunodeficiency virus (HIV) infection [adjusted odds ratio (aOR) = 2.1, 95% CI 1.5-3.0], being SPPTB case (aOR = 3.4, 95% CI 2.4-4.8), being SNPTB case (aOR = 2.0, 95% CI 1.5-2.8)], and being re-treatment cases (aOR = 2.6, 95% CI 1.5-3.7).
Conclusion: In the present study area, there was a high level of adherence to anti-TB treatment and also a high TB treatment success rate. However, still further effort like health education to patient or family is needed to reduce those factors which affect adherence and treatment success rates in order to ensure higher rates of adherence and treatment success than the currently observed in the present study area.
Figures
References
-
- WHO . Global tuberculosis report 2012. WHO/HTM/TB/2012,6. Geneva: Switzerland; 2012.
-
- Volmink J, Garner P. Directly observed therapy for treating tuberculosis. Cochrane Database of Syst Rev. 2007;17:CD003343. - PubMed
-
- Charles P. Felton National Tuberculosis Center. Adherence to Treatment for Latent Tuberculosis Infection. A Manual for Health Care Providers. 2005.
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
