

Is neoadjuvant chemotherapy necessary for patients with initially resectable colorectal liver metastases in the era of effective chemotherapy?
- PMID: 26421041
- PMCID: PMC4582468
- DOI: 10.14701/kjhbps.2011.15.4.206
Is neoadjuvant chemotherapy necessary for patients with initially resectable colorectal liver metastases in the era of effective chemotherapy?
Abstract
Backgrounds/aims: Hepatic resection has only guaranteed long-term survival in patients with colorectal liver metastasis (CRLM) even in the era of effective chemotherapy. The definite role of neoadjuvant chemotherapy (NCT) is to improve outcomes of unresectable CRLMs, but it its role has not been defined for initially resectable CRLMs (IR-CRLMs).
Methods: We reviewed the medical records of 226 patients, who had been diagnosed and treated for IR-CRLM between 2003 and 2008; the patients had the following pathologies: 10% had more than 4 nodules, 11% had tumors larger than 5 cm, and 61% had synchronous CRMLs. Among these patients, 20 patients (Group Y) were treated with NCT, and 206 (Group N) did not receive NCT according to their physician's preference. The median follow-up time was 34.1 months.
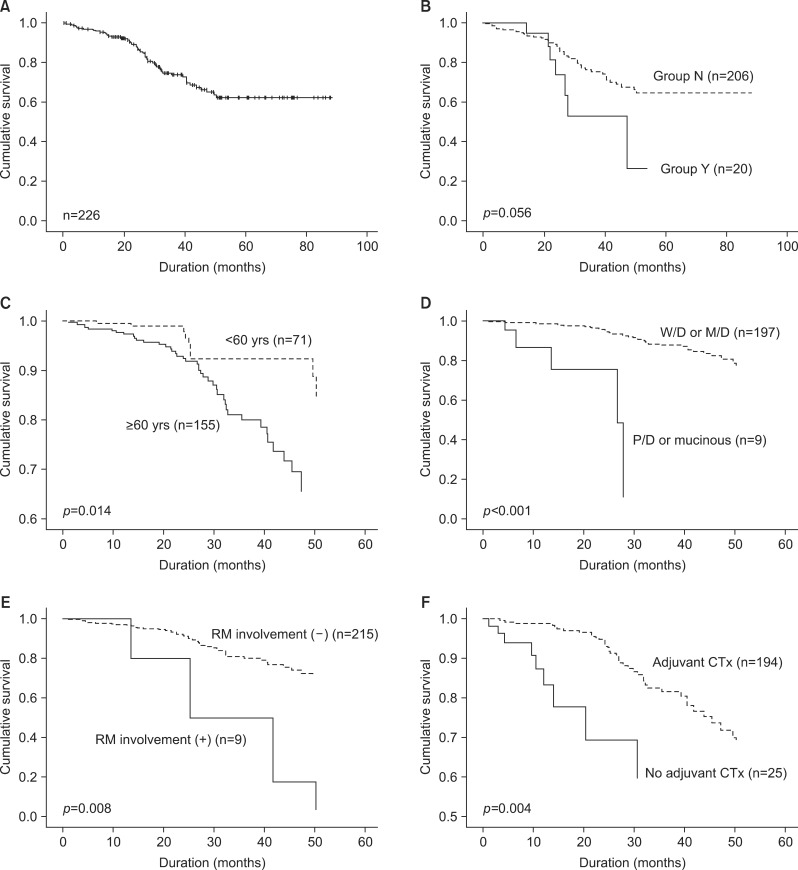
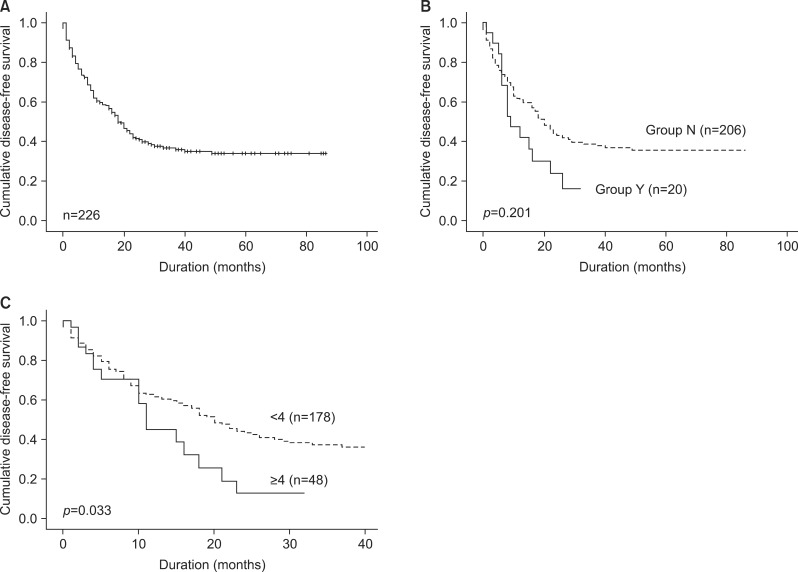
Results: The initial surgical plans were changed after NCT to further resection in 20% and to limited resection in 10% of 20 patients. Complication rates of Groups Y (30%) were indifferent from Group N (23%) (p=0.233), but intraoperative transfusions were more frequent in Group N (15%) than in Group Y (5%) (p=0.006). There was one case of hospital mortality (0.44%). Disease-free survival rates in Groups Y and N were 23% and 39%, respectively, and patient survival rates were 42% and 66% (p>0.05). By multivariate analysis, old age (≥60 years), differentiation of primary tumor (poorly/mucinous), resection margin involvement, and no adjuvant chemotherapy were associated with poor patient survival; the number of CRLMs (≥4) was associated with poor disease-free survival.
Conclusions: NCT had neither a positive impact nor a negative impact on survival, even with intraoperative transfusion, as observed on operative outcomes for patients with IR-CRLM. Further study is required to elucidate the role of NCT for treatment of patient with IR-CRLMs.
Keywords: Adjuvant chemotherapy; Colorectal liver metastasis; Hepatic resection; Neoadjuvant chemotherapy; Prognostic factor.
Figures
Similar articles
-
The clinical relevance of the Fong and the Nordlinger scores in the era of effective neoadjuvant chemotherapy for colorectal liver metastasis.Surg Today. 2015 Dec;45(12):1527-34. doi: 10.1007/s00595-014-1108-9. Epub 2015 Jan 7. Surg Today. 2015. PMID: 25563588
-
Neoadjuvant chemotherapy for colorectal liver metastases: A contemporary review of the literature.World J Gastrointest Oncol. 2021 Sep 15;13(9):1043-1061. doi: 10.4251/wjgo.v13.i9.1043. World J Gastrointest Oncol. 2021. PMID: 34616511 Free PMC article. Review.
-
Adjuvant hepatic arterial infusion pump chemotherapy and resection versus resection alone in patients with low-risk resectable colorectal liver metastases - the multicenter randomized controlled PUMP trial.BMC Cancer. 2019 Apr 5;19(1):327. doi: 10.1186/s12885-019-5515-6. BMC Cancer. 2019. PMID: 30953467 Free PMC article.
-
[Effect of neoadjuvant chemotherapy on the results of resection of colorectal liver metastases].Cir Esp. 2007 Sep;82(3):166-71. doi: 10.1016/s0009-739x(07)71693-7. Cir Esp. 2007. PMID: 17916288 Spanish.
-
OncoSurge: a strategy for long-term survival in metastatic colorectal cancer.Colorectal Dis. 2003 Nov;5 Suppl 3:20-8. doi: 10.1046/j.1463-1318.5.s3.1.x. Colorectal Dis. 2003. PMID: 23573557 Review.
Cited by
-
Neoadjuvant chemotherapy for patients with resectable colorectal cancer liver metastases: A systematic review and meta-analysis.World J Clin Cases. 2021 Aug 6;9(22):6357-6379. doi: 10.12998/wjcc.v9.i22.6357. World J Clin Cases. 2021. PMID: 34435001 Free PMC article.
-
Histopathologic factors affecting tumor recurrence after hepatic resection in colorectal liver metastases.Ann Surg Treat Res. 2014 Jul;87(1):14-21. doi: 10.4174/astr.2014.87.1.14. Epub 2014 Jun 24. Ann Surg Treat Res. 2014. PMID: 25025022 Free PMC article.
References
-
- Nordlinger B, Guiguet M, Vaillant JC, et al. Association Française de Chirurgie. Surgical resection of colorectal carcinoma metastases to the liver. A prognostic scoring system to improve case selection, based on 1568 patients. Cancer. 1996;77:1254–1262. - PubMed
-
- Scheele J, Stang R, Altendorf-Hofmann A, Paul M. Resection of colorectal liver metastases. World J Surg. 1995;19:59–71. - PubMed
-
- House MG, Ito H, Gönen M, et al. Survival after hepatic resection for metastatic colorectal cancer: trends in outcomes for 1,600 patients during two decades at a single institution. J Am Coll Surg. 2010;210:744–752. 752–755. - PubMed
LinkOut - more resources
Full Text Sources