

Unusual Cause of Swelling in the Upper Limb: Kimura Disease
- PMID: 26421119
- PMCID: PMC4576379
- DOI: 10.5001/omj.2015.74
Unusual Cause of Swelling in the Upper Limb: Kimura Disease
Abstract
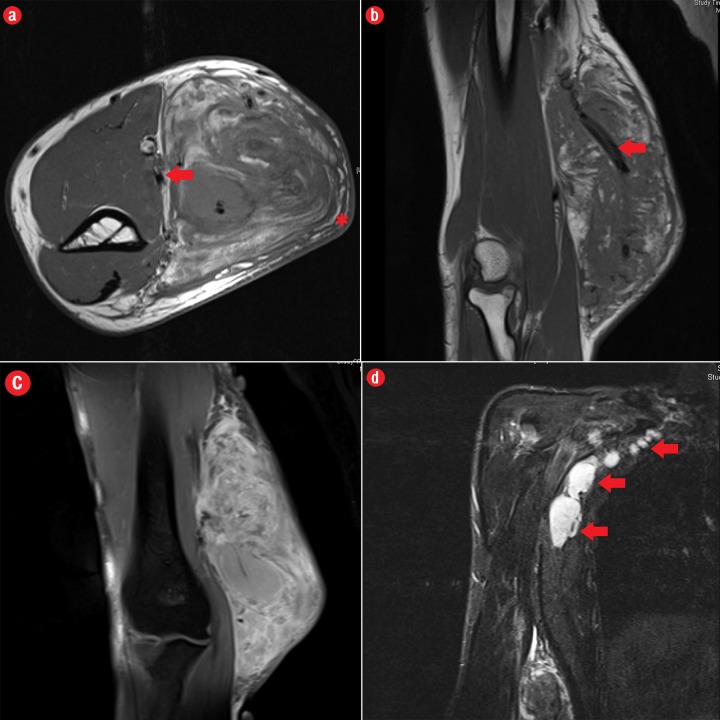
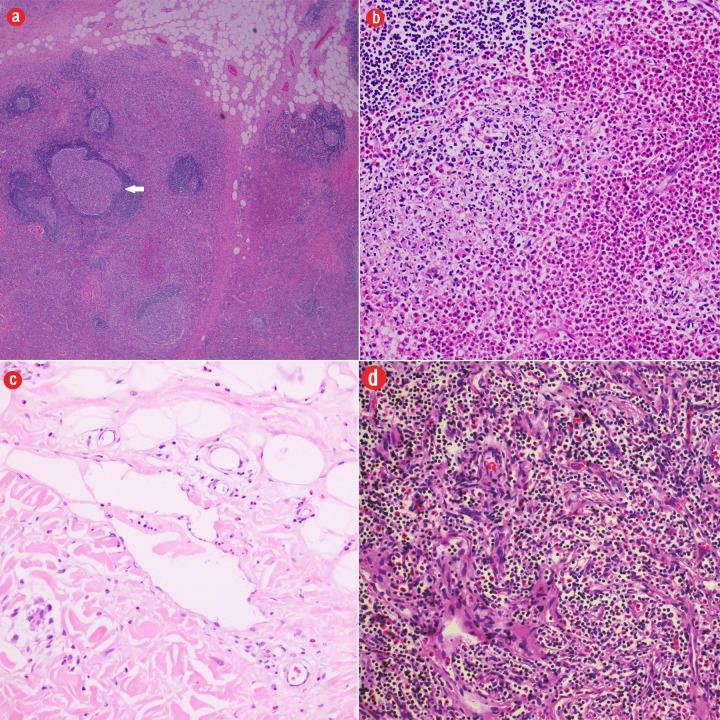
Kimura disease is a rare chronic inflammatory disease of unknown etiology. The disease typically presents in young Asian males with single or multiple slowly progressing painless subcutaneous lumps in the head and neck region; regional lymphadenopathy is commonly accompanied. The disease is associated with peripheral blood eosinophilia and elevated serum immunoglobulin E levels. This gives an important clinical clue to the diagnosis and implies a possible immune-mediated pathophysiology. Although the disease commonly affects the head and neck region, it may also affect the extremities, axilla, groin, and abdomen. Upper limb involvement in Kimura's disease is rare and few cases have been reported in the literature. We describe the case of a man who presented with a history of progressive upper limb swelling. He was diagnosed with Kimura's disease based on concordant clinical, laboratory, radiological, and histopathological grounds. Although rare in the upper limb, the possibility of Kimura's disease has to be considered in young males presenting with painless swelling in the medial epitrochlear region with compatible imaging appearance, particularly if associated with lymph node enlargement and increased blood eosinophils. Characteristic imaging findings of Kimura's disease of the upper limb include specific location along the neuro-lymphovascular structures, the absence of necrosis or calcification, mutliple flow voids representing vascular structures, a varying amount of edema of subcutaneous fat plane overlying the lesion; displacement of adjacent muscles; and neurovascular structures without signs of direct invasion. Clinicians should be aware of this distinct entity in order to avoid misdiagnosis and to tailor appropriate management.
Keywords: Eosinophilia; Kimura Disease; Magnetic Resonance Imaging; Multidetector Computed Tomography; Upper Extremity.
Figures

References
-
- Kimura T, Yoshimura S, Ishikawa E. Unusual granulation combined with hyperplastic changes of lymphatic tissue (in Japanese). Trans Soc Pathol Jpn 1948;37:179-180.
-
- Takagi K, Harada T, Ishikawa E. [Kimura’s disease (eosinophilic lymphfolliculoid granuloma)]. Nihon Rinsho 1993. Mar;51(3):785-788. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Other Literature Sources