

Myocardial Dysfunction and Shock after Cardiac Arrest
- PMID: 26421284
- PMCID: PMC4572400
- DOI: 10.1155/2015/314796
Myocardial Dysfunction and Shock after Cardiac Arrest
Abstract
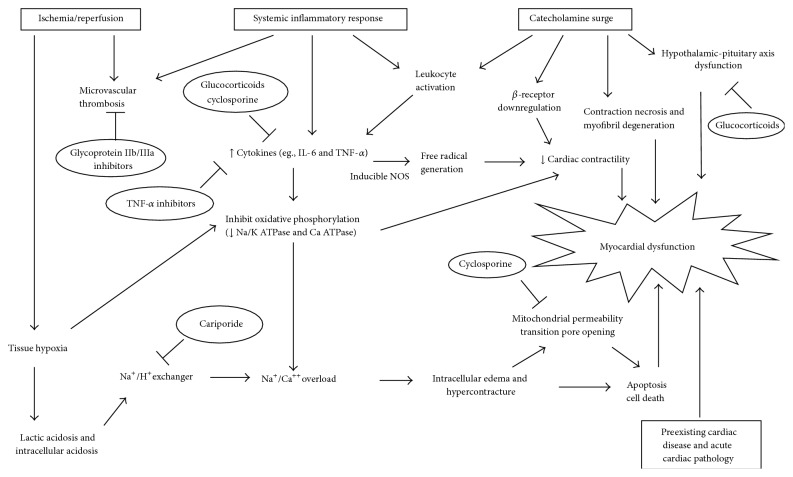
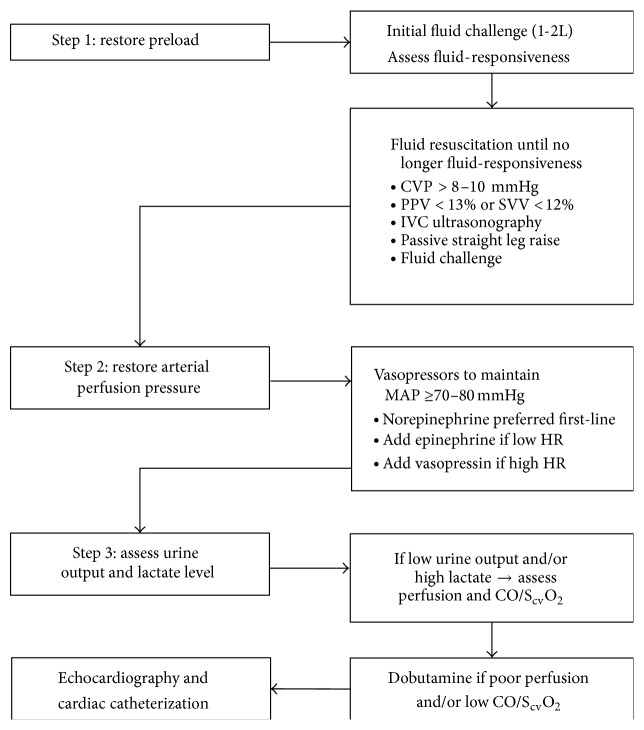
Postarrest myocardial dysfunction includes the development of low cardiac output or ventricular systolic or diastolic dysfunction after cardiac arrest. Impaired left ventricular systolic function is reported in nearly two-thirds of patients resuscitated after cardiac arrest. Hypotension and shock requiring vasopressor support are similarly common after cardiac arrest. Whereas shock requiring vasopressor support is consistently associated with an adverse outcome after cardiac arrest, the association between myocardial dysfunction and outcomes is less clear. Myocardial dysfunction and shock after cardiac arrest develop as the result of preexisting cardiac pathology with multiple superimposed insults from resuscitation. The pathophysiology involves cardiovascular ischemia/reperfusion injury and cardiovascular toxicity from excessive levels of inflammatory cytokine activation and catecholamines, among other contributing factors. Similar mechanisms occur in myocardial dysfunction after cardiopulmonary bypass, in sepsis, and in stress-induced cardiomyopathy. Hemodynamic stabilization after resuscitation from cardiac arrest involves restoration of preload, vasopressors to support arterial pressure, and inotropic support if needed to reverse the effects of myocardial dysfunction and improve systemic perfusion. Further research is needed to define the role of postarrest myocardial dysfunction on cardiac arrest outcomes and identify therapeutic strategies.
Figures
Similar articles
-
The optimal hemodynamics management of post-cardiac arrest shock.Best Pract Res Clin Anaesthesiol. 2015 Dec;29(4):485-95. doi: 10.1016/j.bpa.2015.10.002. Epub 2015 Oct 14. Best Pract Res Clin Anaesthesiol. 2015. PMID: 26670819 Review.
-
Urocortin Treatment Improves Acute Hemodynamic Instability and Reduces Myocardial Damage in Post-Cardiac Arrest Myocardial Dysfunction.PLoS One. 2016 Nov 10;11(11):e0166324. doi: 10.1371/journal.pone.0166324. eCollection 2016. PLoS One. 2016. PMID: 27832152 Free PMC article.
-
Optimum Blood Pressure in Patients With Shock After Acute Myocardial Infarction and Cardiac Arrest.J Am Coll Cardiol. 2020 Aug 18;76(7):812-824. doi: 10.1016/j.jacc.2020.06.043. J Am Coll Cardiol. 2020. PMID: 32792079 Clinical Trial.
-
Apoptosis is not involved in the mechanism of myocardial dysfunction after resuscitation in a rat model of cardiac arrest and cardiopulmonary resuscitation.Crit Care Med. 2010 May;38(5):1329-34. doi: 10.1097/CCM.0b013e3181d9da8d. Crit Care Med. 2010. PMID: 20228676
-
[Pathophysiology and management of post-cardiac arrest syndrome].Ann Fr Anesth Reanim. 2013 Nov;32(11):779-86. doi: 10.1016/j.annfar.2013.07.818. Epub 2013 Oct 15. Ann Fr Anesth Reanim. 2013. PMID: 24138773 Review. French.
Cited by
-
Comparison of Dopamine and Norepinephrine Use for the Treatment of Hypotension in Out-Of-Hospital Cardiac Arrest Patients with Return of Spontaneous Circulation.Emerg Med Int. 2020 Aug 18;2020:7951025. doi: 10.1155/2020/7951025. eCollection 2020. Emerg Med Int. 2020. PMID: 38264544 Free PMC article.
-
Prevalence of Torsades de Pointes inducing drugs usage among elderly outpatients in North Jordan Hospitals.Saudi Pharm J. 2018 Dec;26(8):1146-1154. doi: 10.1016/j.jsps.2018.07.002. Epub 2018 Jul 29. Saudi Pharm J. 2018. PMID: 30532635 Free PMC article.
-
Impaired echocardiographic left ventricular global longitudinal strain after pediatric cardiac arrest children is associated with mortality.Resuscitation. 2023 Oct;191:109936. doi: 10.1016/j.resuscitation.2023.109936. Epub 2023 Aug 11. Resuscitation. 2023. PMID: 37574003 Free PMC article.
-
Effect of therapeutic hypothermia against renal injury in a rat model of asphyxial cardiac arrest: Α focus on the survival rate, pathophysiology and antioxidant enzymes.Mol Med Rep. 2022 Jan;25(1):19. doi: 10.3892/mmr.2021.12535. Epub 2021 Nov 19. Mol Med Rep. 2022. PMID: 34796906 Free PMC article.
-
Multidisciplinary Critical Care Management of Electrical Storm: JACC State-of-the-Art Review.J Am Coll Cardiol. 2023 Jun 6;81(22):2189-2206. doi: 10.1016/j.jacc.2023.03.424. J Am Coll Cardiol. 2023. PMID: 37257955 Free PMC article. Review.
References
-
- McNally B., Robb R., Mehta M., et al. Out-of-hospital cardiac arrest surveillance—cardiac arrest registry to enhance survival (CARES), United States, October 1, 2005–December 31, 2010. Morbidity and Mortality Weekly Report: Surveillance Summaries. 2011;60:1–19. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
