

Agent-Based Model Forecasts Aging of the Population of People Who Inject Drugs in Metropolitan Chicago and Changing Prevalence of Hepatitis C Infections
- PMID: 26421722
- PMCID: PMC4589282
- DOI: 10.1371/journal.pone.0137993
Agent-Based Model Forecasts Aging of the Population of People Who Inject Drugs in Metropolitan Chicago and Changing Prevalence of Hepatitis C Infections
Abstract
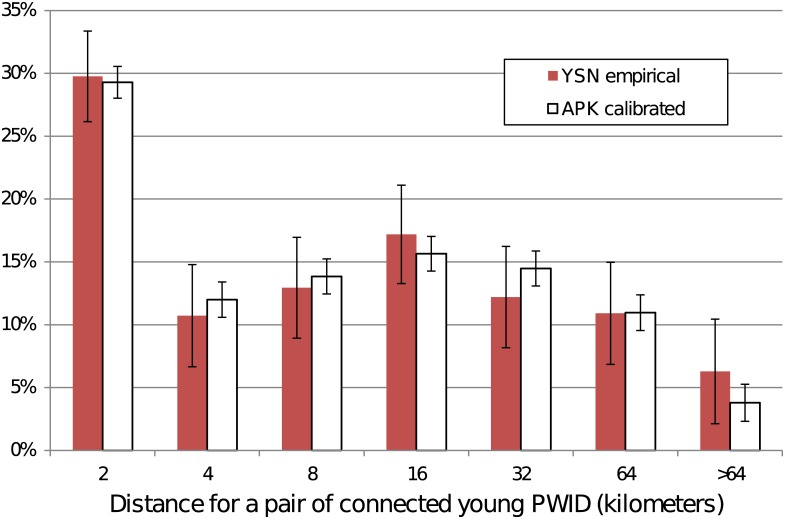
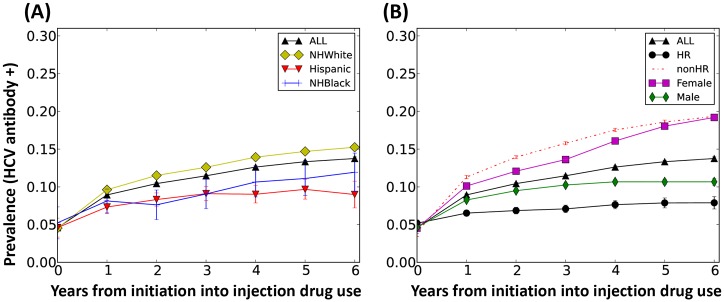
People who inject drugs (PWID) are at high risk for blood-borne pathogens transmitted during the sharing of contaminated injection equipment, particularly hepatitis C virus (HCV). HCV prevalence is influenced by a complex interplay of drug-use behaviors, social networks, and geography, as well as the availability of interventions, such as needle exchange programs. To adequately address this complexity in HCV epidemic forecasting, we have developed a computational model, the Agent-based Pathogen Kinetics model (APK). APK simulates the PWID population in metropolitan Chicago, including the social interactions that result in HCV infection. We used multiple empirical data sources on Chicago PWID to build a spatial distribution of an in silico PWID population and modeled networks among the PWID by considering the geography of the city and its suburbs. APK was validated against 2012 empirical data (the latest available) and shown to agree with network and epidemiological surveys to within 1%. For the period 2010-2020, APK forecasts a decline in HCV prevalence of 0.8% per year from 44(± 2)% to 36(± 5)%, although some sub-populations would continue to have relatively high prevalence, including Non-Hispanic Blacks, 48(± 5)%. The rate of decline will be lowest in Non-Hispanic Whites and we find, in a reversal of historical trends, that incidence among non-Hispanic Whites would exceed incidence among Non-Hispanic Blacks (0.66 per 100 per years vs 0.17 per 100 person years). APK also forecasts an increase in PWID mean age from 35(± 1) to 40(± 2) with a corresponding increase from 59(± 2)% to 80(± 6)% in the proportion of the population >30 years old. Our studies highlight the importance of analyzing subpopulations in disease predictions, the utility of computer simulation for analyzing demographic and health trends among PWID and serve as a tool for guiding intervention and prevention strategies in Chicago, and other major cities.
Conflict of interest statement
Figures








References
-
- WHO. World Health Organization. Hepatitis C Fact Sheet No 164. 2015 Available: http://www.who.int/mediacentre/factsheets/fs164/en/.
-
- CDC. Centers for Disease Control and Prevention. HCV statistics. 2014 Available: http://www.cdc.gov/hepatitis/HCV/StatisticsHCV.htm.
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
