

Effect of a Cognitive-Behavioral Prevention Program on Depression 6 Years After Implementation Among At-Risk Adolescents: A Randomized Clinical Trial
- PMID: 26421861
- PMCID: PMC4635056
- DOI: 10.1001/jamapsychiatry.2015.1559
Effect of a Cognitive-Behavioral Prevention Program on Depression 6 Years After Implementation Among At-Risk Adolescents: A Randomized Clinical Trial
Abstract
Importance: Adolescents whose parents have a history of depression are at risk for developing depression and functional impairment. The long-term effects of prevention programs on adolescent depression and functioning are not known.
Objective: To determine whether a cognitive-behavioral prevention (CBP) program reduced the incidence of depressive episodes, increased depression-free days, and improved developmental competence 6 years after implementation.
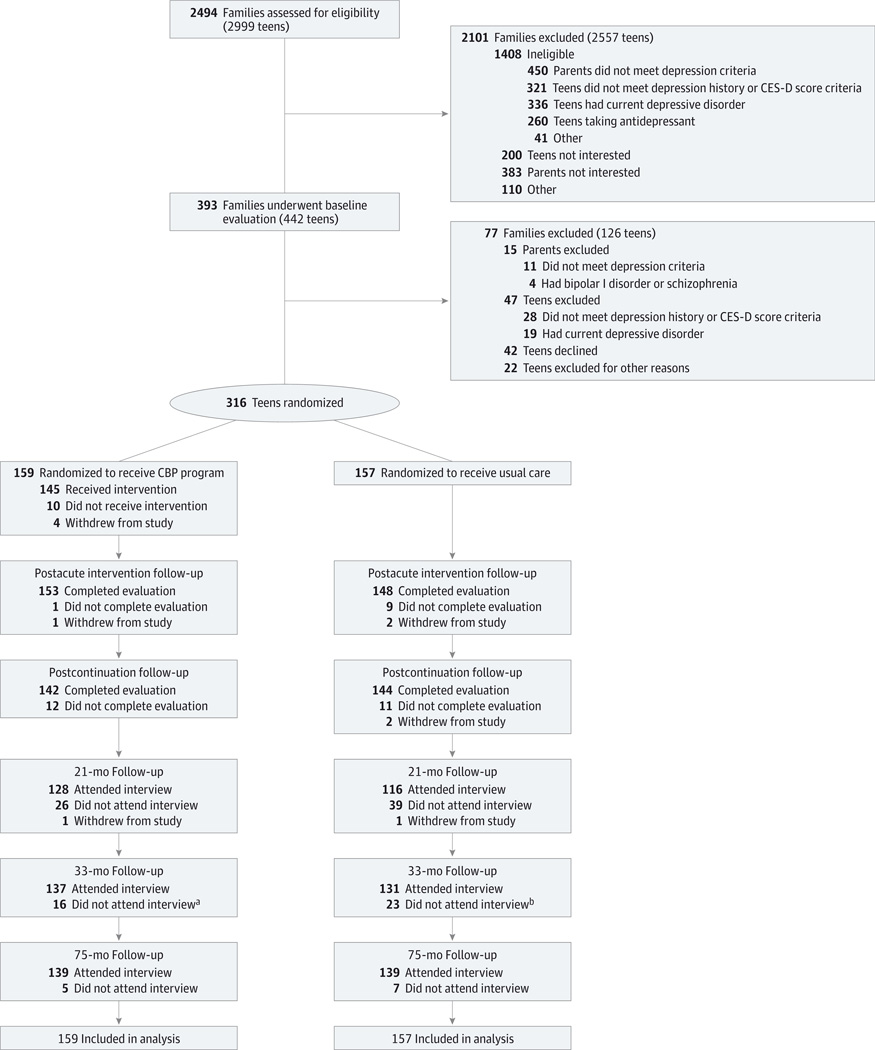
Design, setting, and participants: A 4-site randomized clinical trial compared the effect of CBP plus usual care vs usual care, through follow-up 75 months after the intervention (88% retention), with recruitment from August 2003 through February 2006 at a health maintenance organization, university medical centers, and a community mental health center. A total of 316 participants were 13 to 17 years of age at enrollment and had at least 1 parent with current or prior depressive episodes. Participants could not be in a current depressive episode but had to have subsyndromal depressive symptoms or a prior depressive episode currently in remission. Analysis was conducted between August 2014 and June 2015.
Interventions: The CBP program consisted of 8 weekly 90-minute group sessions followed by 6 monthly continuation sessions. Usual care consisted of any family-initiated mental health treatment.
Main outcomes and measures: The Depression Symptoms Rating scale was used to assess the primary outcome, new onsets of depressive episodes, and to calculate depression-free days. A modified Status Questionnaire assessed developmental competence (eg, academic or interpersonal) in young adulthood.
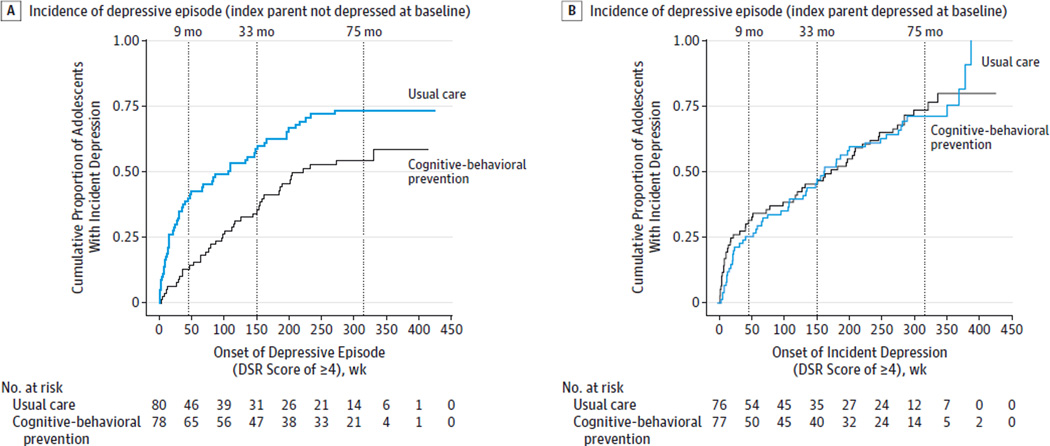
Results: Over the 75-month follow-up, youths assigned to CBP had a lower incidence of depression, adjusting for current parental depression at enrollment, site, and all interactions (hazard ratio, 0.71 [95% CI, 0.53-0.96]). The CBP program's overall significant effect was driven by a lower incidence of depressive episodes during the first 9 months after enrollment. The CBP program's benefit was seen in youths whose index parent was not depressed at enrollment, on depression incidence (hazard ratio, 0.54 [95% CI, 0.36-0.81]), depression-free days (d = 0.34, P = .01), and developmental competence (d = 0.36, P = .04); these effects on developmental competence were mediated via the CBP program's effect on depression-free days.
Conclusions and relevance: The effect of CBP on new onsets of depression was strongest early and was maintained throughout the follow-up period; developmental competence was positively affected 6 years later. The effectiveness of CBP may be enhanced by additional booster sessions and concomitant treatment of parental depression.
Trial registration: clinicaltrials.gov Identifier:NCT00073671.
Conflict of interest statement
Figures

Comment in
-
Long-term benefits of cognitive-behavioural prevention for adolescents at risk of depression but not if parents are depressed at the onset of the programme.Evid Based Ment Health. 2016 Aug;19(3):e20. doi: 10.1136/eb-2016-102323. Epub 2016 Jun 24. Evid Based Ment Health. 2016. PMID: 27343019 Free PMC article. No abstract available.
References
Publication types
MeSH terms
Associated data
Grants and funding
- T32MH018921/MH/NIMH NIH HHS/United States
- UL1 TR000445/TR/NCATS NIH HHS/United States
- R01 MH64717/MH/NIMH NIH HHS/United States
- R01 MH064735/MH/NIMH NIH HHS/United States
- R01 MH64541/MH/NIMH NIH HHS/United States
- R01 MH064541/MH/NIMH NIH HHS/United States
- T32 MH018921/MH/NIMH NIH HHS/United States
- U54 HD083211/HD/NICHD NIH HHS/United States
- R01MH064735/MH/NIMH NIH HHS/United States
- 2 UL1 TR000445-06/TR/NCATS NIH HHS/United States
- R01 MH064503/MH/NIMH NIH HHS/United States
- R01 MH064717/MH/NIMH NIH HHS/United States
- K12 HS022990/HS/AHRQ HHS/United States
- R01 MH64503/MH/NIMH NIH HHS/United States
- UL1 RR024975/RR/NCRR NIH HHS/United States
- UL1 RR024975-01/RR/NCRR NIH HHS/United States
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
