

Magnitude of Treatment Abandonment in Childhood Cancer
- PMID: 26422208
- PMCID: PMC4589240
- DOI: 10.1371/journal.pone.0135230
Magnitude of Treatment Abandonment in Childhood Cancer
Abstract
Background: Treatment abandonment (TxA) is recognized as a leading cause of treatment failure for children with cancer in low-and-middle-income countries (LMC). However, its global frequency and burden have remained elusive due to lack of global data. This study aimed to obtain an estimate using survey and population data.
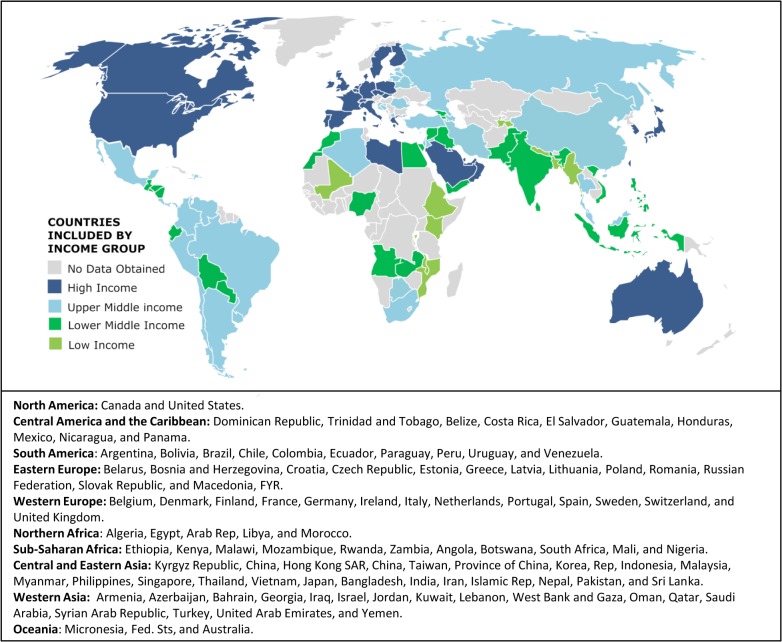
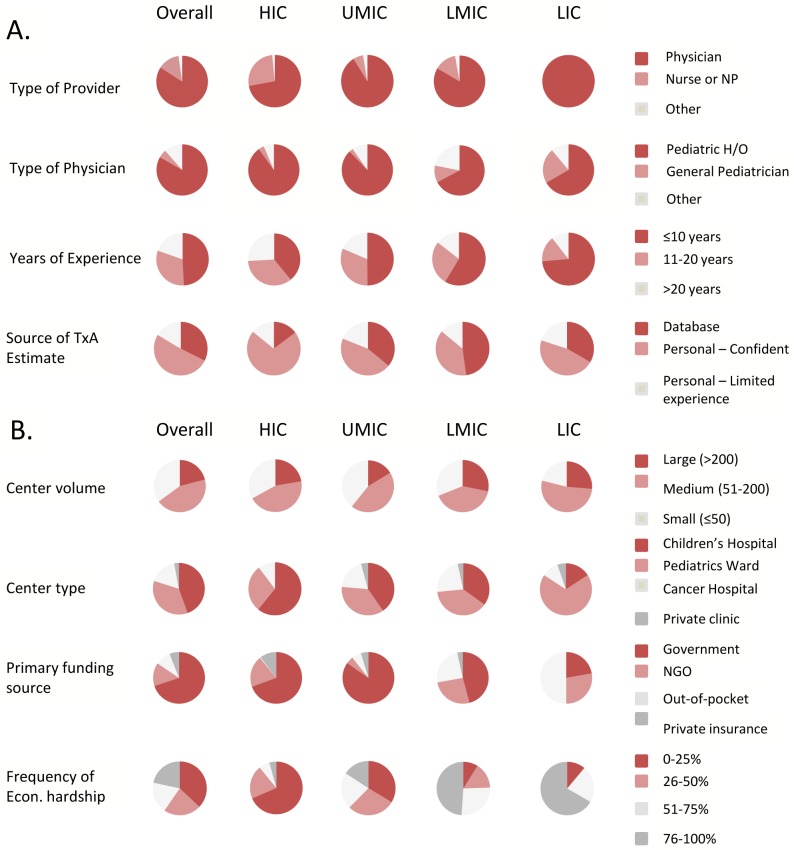
Methods: Childhood cancer clinicians (medical oncologists, surgeons, and radiation therapists), nurses, social workers, and psychologists involved in care of children with cancer were approached through an online survey February-May 2012. Incidence and population data were obtained from public sources. Descriptive, univariable, and multivariable analyses were conducted.
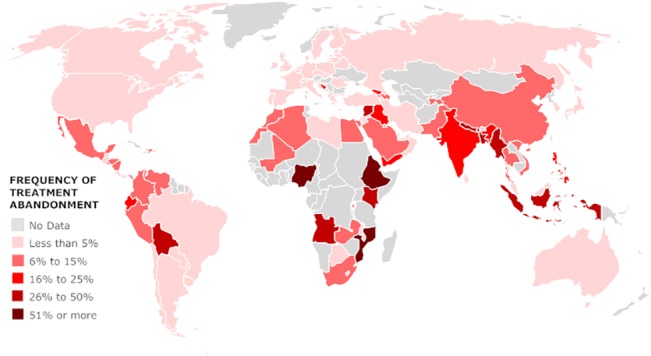
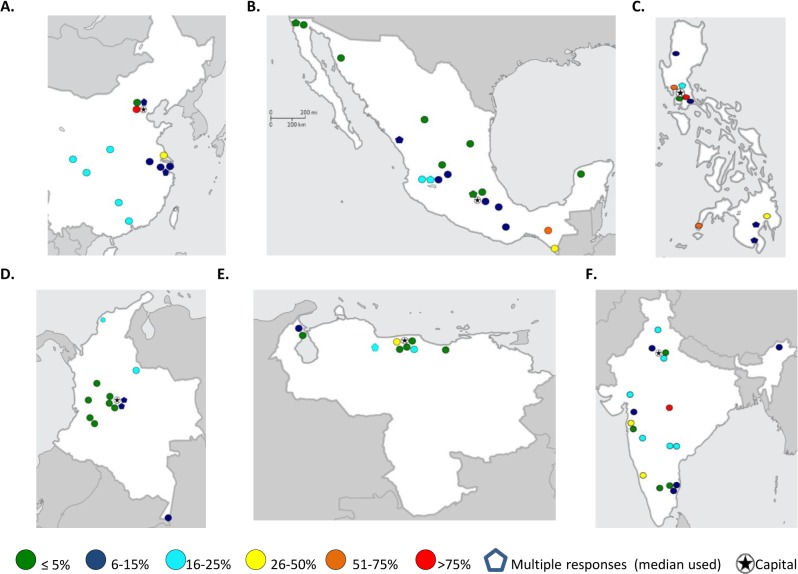
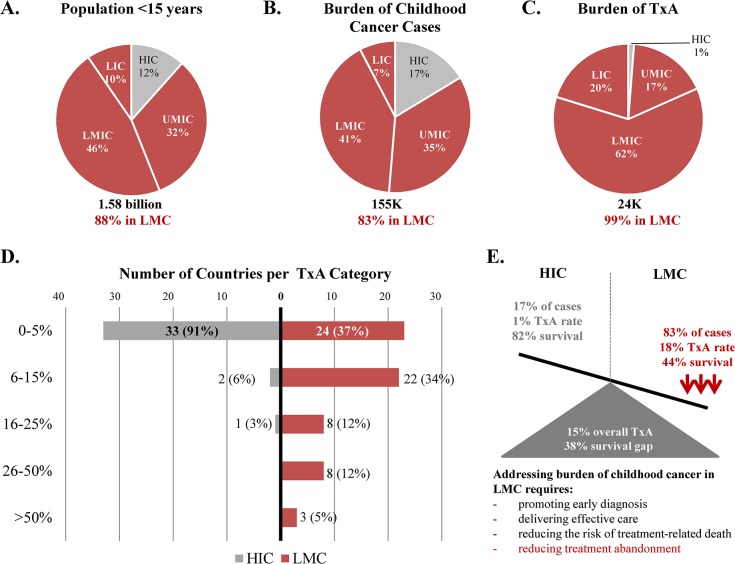
Results: 602 responses from 101 countries were obtained from physicians (84%), practicing pediatric hematology/oncology (83%) in general or children's hospitals (79%). Results suggested, 23,854 (15%) of 155,088 children <15 years old newly diagnosed with cancer annually in the countries analyzed, abandon therapy. Importantly, 83% of new childhood cancer cases and 99% of TxA were attributable to LMC. The annual number of cases of TxA expected in LMC worldwide (26,166) was nearly equivalent to the annual number of cancer cases in children <15 years expected in HIC (26,368). Approximately two thirds of LMC had median TxA ≥ 6%, but TxA ≥ 6% was reported in high- (9%), upper-middle- (41%), lower-middle- (80%), and low-income countries (90%, p<0.001). Most LMC centers reporting TxA > 6% were outside the capital. Lower national income category, higher reliance on out-of-pocket payments, and high prevalence of economic hardship at the center were independent contextual predictors for TxA ≥ 6% (p<0.001). Global survival data available for more developed and less developed regions suggests TxA may account for at least a third of the survival gap between HIC and LMC.
Conclusion: Results show TxA is prevalent (compromising cancer survival for 1 in 7 children globally), confirm the suspected high burden of TxA in LMC, and illustrate the negative impact of poverty on its occurrence. The present estimates may appear small compared to the global burden of child death from malnutrition and infection (measured in millions). However, absolute numbers suggest the burden of TxA in LMC is nearly equivalent to annually losing all kids diagnosed with cancer in HIC just to TxA, without even considering deaths from disease progression, relapse or toxicity-the main causes of childhood cancer mortality in HIC. Results document the importance of monitoring and addressing TxA as part of childhood cancer outcomes in at-risk settings.
Conflict of interest statement
Figures
References
-
- Hord JD, Rehman W, Hannon P, Anderson-Shaw L, Schmidt ML. Do parents have the right to refuse standard treatment for their child with favorable-prognosis cancer? Ethical and legal concerns. J Clin Oncol. 2006;24(34):5454–6. Epub 2006/12/01. doi: 24/34/5454 [pii] 10.1200/JCO.2006.06.4709 . - DOI - PubMed
-
- Lam CG, Rossell N, RC R. Global Snapshots of Treatment Abandonment in Children and Adolescents with Cancer: Social Factors, Implications, and Priorities. J Healthcare, Science and Humanities 2012;2(1):81–110.
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
