

Does Publication Bias Inflate the Apparent Efficacy of Psychological Treatment for Major Depressive Disorder? A Systematic Review and Meta-Analysis of US National Institutes of Health-Funded Trials
- PMID: 26422604
- PMCID: PMC4589340
- DOI: 10.1371/journal.pone.0137864
Does Publication Bias Inflate the Apparent Efficacy of Psychological Treatment for Major Depressive Disorder? A Systematic Review and Meta-Analysis of US National Institutes of Health-Funded Trials
Abstract
Background: The efficacy of antidepressant medication has been shown empirically to be overestimated due to publication bias, but this has only been inferred statistically with regard to psychological treatment for depression. We assessed directly the extent of study publication bias in trials examining the efficacy of psychological treatment for depression.
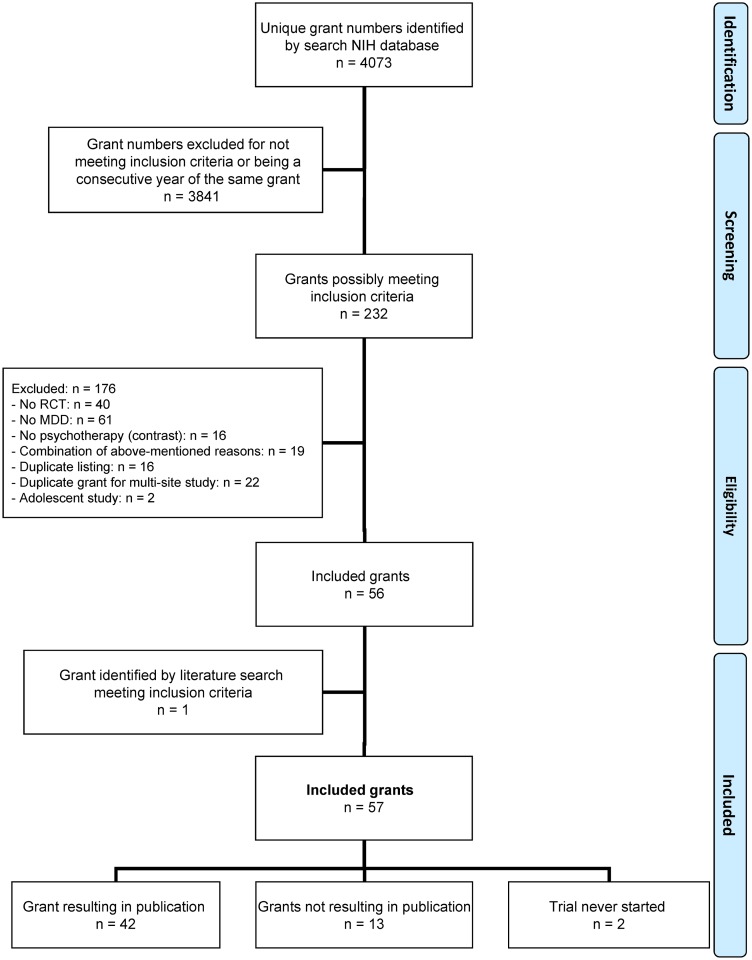
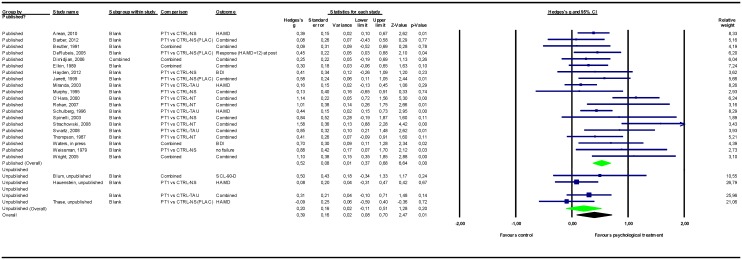
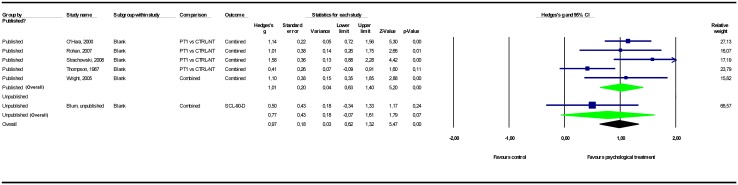
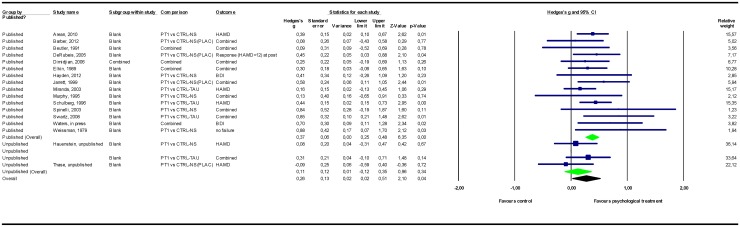
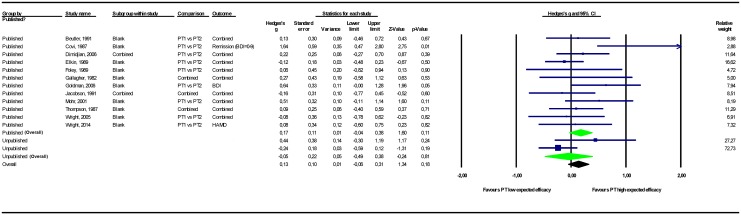
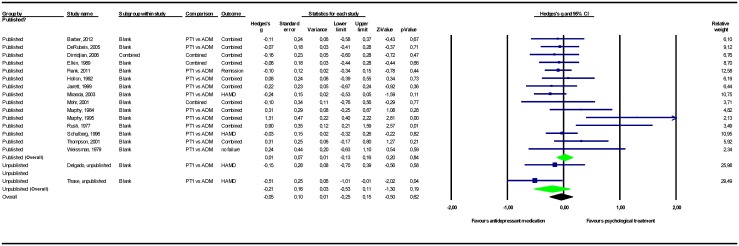
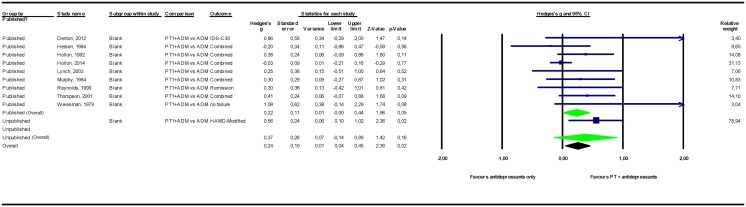
Methods and findings: We identified US National Institutes of Health grants awarded to fund randomized clinical trials comparing psychological treatment to control conditions or other treatments in patients diagnosed with major depressive disorder for the period 1972-2008, and we determined whether those grants led to publications. For studies that were not published, data were requested from investigators and included in the meta-analyses. Thirteen (23.6%) of the 55 funded grants that began trials did not result in publications, and two others never started. Among comparisons to control conditions, adding unpublished studies (Hedges' g = 0.20; CI95% -0.11~0.51; k = 6) to published studies (g = 0.52; 0.37~0.68; k = 20) reduced the psychotherapy effect size point estimate (g = 0.39; 0.08~0.70) by 25%. Moreover, these findings may overestimate the "true" effect of psychological treatment for depression as outcome reporting bias could not be examined quantitatively.
Conclusion: The efficacy of psychological interventions for depression has been overestimated in the published literature, just as it has been for pharmacotherapy. Both are efficacious but not to the extent that the published literature would suggest. Funding agencies and journals should archive both original protocols and raw data from treatment trials to allow the detection and correction of outcome reporting bias. Clinicians, guidelines developers, and decision makers should be aware that the published literature overestimates the effects of the predominant treatments for depression.
Conflict of interest statement
Figures
Comment in
-
[Psychotherapeutic treatments in major depression: the literature shows a very optimistic picture].Rev Med Suisse. 2015 Nov 18;11(495):2200. Rev Med Suisse. 2015. PMID: 26742246 French. No abstract available.
References
-
- Dickersin K. The existence of publication bias and risk factors for its occurrence. JAMA. 1990;263: 1385–1389. - PubMed
-
- Rosenthal R. The “file drawer problem” and tolerance for null results. Psychol Bull. 1979;86: 638–641.
-
- Kessler RC, Berglund P, Demler O, Jin R, Koretz D, Merikangas KR, et al. The epidemiology of major depressive disorder: Results from the National Comorbidity Survey Replication (NCS-R). JAMA. 2003;289: 3095–3105. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
