

Efficacy, safety, and tolerability of augmentation pharmacotherapy with aripiprazole for treatment-resistant depression in late life: a randomised, double-blind, placebo-controlled trial
- PMID: 26423182
- PMCID: PMC4690746
- DOI: 10.1016/S0140-6736(15)00308-6
Efficacy, safety, and tolerability of augmentation pharmacotherapy with aripiprazole for treatment-resistant depression in late life: a randomised, double-blind, placebo-controlled trial
Erratum in
- Lancet. 2015 Dec 12;386(10011):2394
-
Department of Error.Lancet. 2025 May 31;405(10493):1908. doi: 10.1016/S0140-6736(25)01102-X. Lancet. 2025. PMID: 40449970 No abstract available.
Abstract
Background: Treatment-resistant major depression is common and potentially life-threatening in elderly people, in whom little is known about the benefits and risks of augmentation pharmacotherapy. We aimed to assess whether aripiprazole is associated with a higher probability of remission than is placebo.
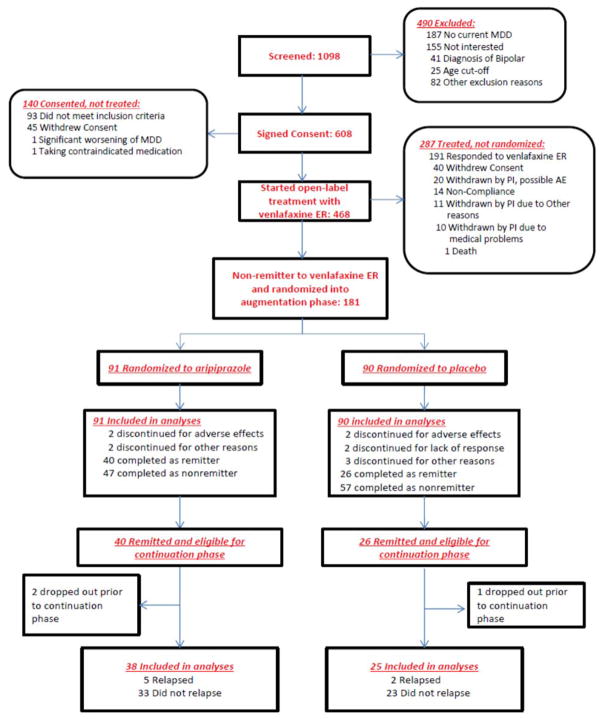
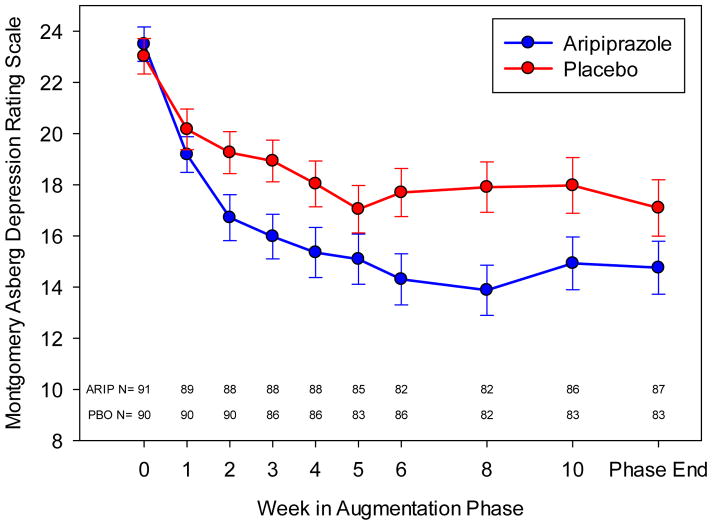
Methods: We did a randomised, double-blind, placebo-controlled trial at three centres in the USA and Canada to test the efficacy and safety of aripiprazole augmentation for adults aged older than 60 years with treatment-resistant depression (Montgomery Asberg Depression Rating Scale [MADRS] score of ≥15). Patients who did not achieve remission during a pre-trial with venlafaxine extended-release (150-300 mg/day) were randomly assigned (1:1) to the addition of aripiprazole (target dose 10 mg [maximum 15 mg] daily) daily or placebo for 12 weeks. The computer-generated randomisation was done in blocks and stratified by site. Only the database administrator and research pharmacists had knowledge of treatment assignment. The primary endpoint was remission, defined as an MADRS score of 10 or less (and at least 2 points below the score at the start of the randomised phase) at both of the final two consecutive visits, analysed by intention to treat. This trial is registered with ClinicalTrials.gov, number NCT00892047.
Findings: From July 20, 2009, to Dec 30, 2013, we recruited 468 eligible participants, 181 (39%) of whom did not remit and were randomly assigned to aripiprazole (n=91) or placebo (n=90). A greater proportion of participants in the aripiprazole group achieved remission than did those in the placebo group (40 [44%] vs 26 [29%] participants; odds ratio [OR] 2·0 [95% CI 1·1-3·7], p=0·03; number needed to treat [NNT] 6·6 [95% CI 3·5-81·8]). Akathisia was the most common adverse effect of aripiprazole (reported in 24 [26%] of 91 participants on aripiprazole vs 11 [12%] of 90 on placebo). Compared with placebo, aripiprazole was also associated with more Parkinsonism (15 [17%] of 86 vs two [2%] of 81 participants), but not with treatment-emergent suicidal ideation (13 [21%] of 61 vs 19 [29%] of 65 participants) or other measured safety variables.
Interpretation: In adults aged 60 years or older who do not achieve remission from depression with a first-line antidepressant, the addition of aripiprazole is effective in achieving and sustaining remission. Tolerability concerns include the potential for akathisia and Parkinsonism.
Funding: National Institute of Mental Health, UPMC Endowment in Geriatric Psychiatry, Taylor Family Institute for Innovative Psychiatric Research, National Center for Advancing Translational Sciences, and the Campbell Family Mental Health Research Institute.
Copyright © 2015 Elsevier Ltd. All rights reserved.
Conflict of interest statement
Dr. Mulsant currently receives research funding from Brain Canada, the CAMH Foundation, the Canadian Institutes of Health Research, and the US National Institute of Health (NIH). During the last five years, he also received research support from Bristol-Myers Squibb (medications for a NIH-funded clinical trial), Eli-Lilly (medications for a NIH-funded clinical trial), and Pfizer (medications for a NIH-funded clinical trial). He directly owns stocks of General Electric (less than $5,000).
Dr. Blumberger has received research support from the Canadian Institutes of Health Research (CIHR), Brain and Behavior Research Foundation (formerly NARSAD), National Institute of Health (NIH), Temerty Family through the Centre for Addiction and Mental Health (CAMH) Foundation and the Campbell Research Institute. He receives research support and in-kind equipment support for an investigator-initiated study from Brainsway Ltd. and he is the site principal investigator for three sponsor-initiated studies for Brainsway Ltd. He also receives in-kind equipment support from Magventure for an investigator-initiated study. None the above represent a conflict of interest with manuscript under consideration.
Dr. Karp has received medication supplies for investigator initiated trials from Pfizer and Reckitt Benckiser.
Dr. Newcomer reports Data Safety Monitoring Board for Bristol-Myers Squibb, Data Safety Monitoring Board for Merck, honoraria from VIVUS, Data Safety Monitoring Board from Amgen.
Dr. Anderson reports receiving grant support from the NIH grants P30 MH090333, R01 MH090250, R01 MH084921.
Dr. Dew receives grant support from the National Institutes of Health, and serves on the editorial boards of numerous clinical journals. None of these activities represent a conflict of interest with the manuscript under consideration.
Dr. Butters has received research support from the National Institutes of Health. She served as a consultant for Medtronic and Northstar Neuroscience from whom she received remuneration for neuropsychological evaluations performed within the context of clinical trials. She also served as a consultant for GlaxoSmithKline, from whom she received remuneration for participating in cognitive disorder diagnostic consensus conferences for research participants in a clinical trial. None of the above represents a conflict of interest with the manuscript under consideration.
Ms. Stack and Ms. Begley report no conflicts.
Dr. Reynolds reports receiving pharmaceutical support for NIH-sponsored research studies from Bristol-Myers Squibb, Forest, Pfizer, and Lilly; receiving grants from the National Institute of Mental Health, National Institute on Aging, National Center for Minority Health Disparities, National Heart Lung and Blood Institute, Center for Medicare and Medicaid Services (CMS), Patient Centered Outcomes Research Institute (PCORI), the Commonwealth of Pennsylvania, the John A Hartford Foundation, National Palliative Care Research Center (NPCRC), Clinical and Translational Science Institute (CTSI), and the American Foundation for Suicide Prevention; and serving on the American Association for Geriatric Psychiatry editorial review board. He has received an honorarium as a speaker from MedScape/WEB MD. He is the co-inventor (Licensed Intellectual Property) of Psychometric analysis of the Pittsburgh Sleep Quality Index (PSQI) PRO10050447 (PI: Buysse).
Figures
Comment in
-
Management of late-life depression: a major leap forward.Lancet. 2015 Dec 12;386(10011):2374-5. doi: 10.1016/S0140-6736(15)00304-9. Epub 2015 Sep 27. Lancet. 2015. PMID: 26423179 No abstract available.
-
ACP Journal Club. In older adults with treatment-resistant depression, adding aripiprazole to venlafaxine increased remission at 12 wk.Ann Intern Med. 2016 Jan 19;164(2):JC10. doi: 10.7326/ACPJC-2016-164-2-010. Ann Intern Med. 2016. PMID: 26784490 No abstract available.
References
-
- Whiteford HA, Degenhardt L, Rehm J, Baxter AJ, Ferrari AJ, Erskine HE, et al. Global burden of disease attributable to mental and substance use disorders: findings from the Global Burden of Disease Study 2010. Lancet. 2013;382(9904):1575–86. - PubMed
-
- Callahan CM, Kroenke K, Counsell SR, Hendrie HC, Perkins AJ, Katon W, et al. Treatment of depression improves physical functioning in older adults. J Am Geriatr Soc. 2005;53(3):367–73. - PubMed
-
- Bruce ML, Ten Have TR, Reynolds CF, 3rd, Katz II, Schulberg HC, Mulsant BH, et al. Reducing suicidal ideation and depressive symptoms in depressed older primary care patients: a randomized controlled trial. JAMA. 2004;291(9):1081–91. - PubMed
-
- Conwell Y, Duberstein PR, Caine ED. Risk factors for suicide in later life. Biol Psychiatry. 2002;52(3):193–204. - PubMed
Publication types
MeSH terms
Substances
Associated data
Grants and funding
- P30 AG024827/AG/NIA NIH HHS/United States
- UL1 TR000005/TR/NCATS NIH HHS/United States
- P30 MH090333/MH/NIMH NIH HHS/United States
- R01 MH083660/MH/NIMH NIH HHS/United States
- R01 MH083648/MH/NIMH NIH HHS/United States
- P30 MH90333/MH/NIMH NIH HHS/United States
- R01 AG049369/AG/NIA NIH HHS/United States
- R01 MH083643/MH/NIMH NIH HHS/United States
- UL1 TR000448/TR/NCATS NIH HHS/United States
- KL2 TR000146/TR/NCATS NIH HHS/United States
- R01 MH090250/MH/NIMH NIH HHS/United States
- R01 MH084921/MH/NIMH NIH HHS/United States
LinkOut - more resources
Full Text Sources
Medical
Research Materials
