

Monitoring and switching of first-line antiretroviral therapy in adult treatment cohorts in sub-Saharan Africa: collaborative analysis
- PMID: 26423252
- PMCID: PMC4500741
- DOI: 10.1016/S2352-3018(15)00087-9
Monitoring and switching of first-line antiretroviral therapy in adult treatment cohorts in sub-Saharan Africa: collaborative analysis
Abstract
Background: HIV-1 viral load testing is recommended to monitor antiretroviral therapy (ART) but is not universally available. The aim of our study was to assess monitoring of first-line ART and switching to second-line ART in sub-Saharan Africa.
Methods: We did a collaborative analysis of cohort studies from 16 countries in east Africa, southern Africa, and west Africa that participate in the international epidemiological database to evaluate AIDS (IeDEA). We included adults infected with HIV-1 who started combination ART between January, 2004, and January, 2013. We defined switching of ART as a change from a non-nucleoside reverse-transcriptase inhibitor (NNRTI)-based regimen to one including a protease inhibitor, with adjustment of one or more nucleoside reverse-transcriptase inhibitors (NRTIs). Virological and immunological failures were defined according to WHO criteria. We calculated cumulative probabilities of switching and hazard ratios with 95% CIs comparing routine viral load monitoring, targeted viral load monitoring, CD4 monitoring, and clinical monitoring, adjusting for programme and individual characteristics.
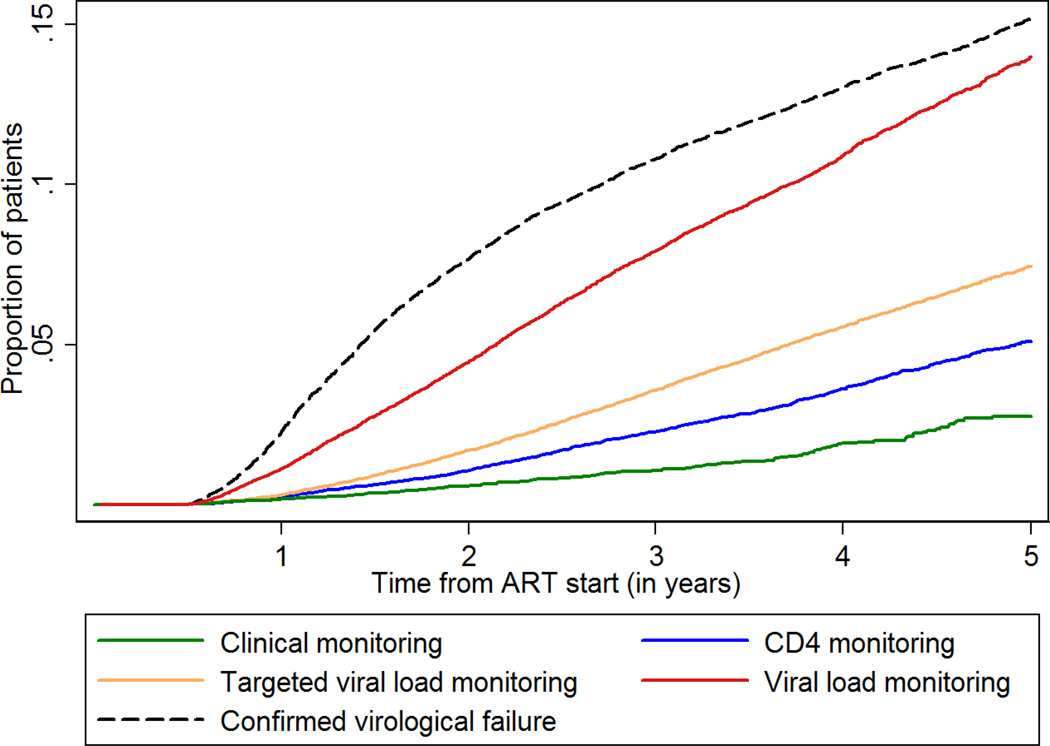
Findings: Of 297,825 eligible patients, 10,352 (3%) switched to second-line ART during 782 ,412 person-years of follow-up. Compared with CD4 monitoring, hazard ratios for switching were 3·15 (95% CI 2·92-3·40) for routine viral load monitoring, 1·21 (1·13-1·30) for targeted viral load monitoring, and 0·49 (0·43-0·56) for clinical monitoring. Of 6450 patients with confirmed virological failure, 58·0% (95% CI 56·5-59·6) switched by 2 years, and of 15,892 patients with confirmed immunological failure, 19·3% (18·5-20·0) switched by 2 years. Of 10,352 patients who switched, evidence of treatment failure based on one CD4 count or viral load measurement ranged from 86 (32%) of 268 patients with clinical monitoring to 3754 (84%) of 4452 with targeted viral load monitoring. Median CD4 counts at switching were 215 cells per μL (IQR 117-335) with routine viral load monitoring, but were lower with other types of monitoring (range 114-133 cells per μL).
Interpretation: Overall, few patients switched to second-line ART and switching happened late in the absence of routine viral load monitoring. Switching was more common and happened earlier after initiation of ART with targeted or routine viral load testing.
Funding: National Institute of Allergy and Infectious Diseases, Swiss National Science Foundation.
Copyright © 2015 Elsevier Ltd. All rights reserved.
Conflict of interest statement
We declare that we have no conflicts of interest.
Figures
Comment in
-
ART in sub-Saharan Africa: the value of viral load monitoring.Lancet HIV. 2015 Jul;2(7):e261-2. doi: 10.1016/S2352-3018(15)00109-5. Epub 2015 Jun 16. Lancet HIV. 2015. PMID: 26423247 No abstract available.
References
-
- World Health Organization. HIV/AIDS. Data and statistics. [accessed April 8, 2015];2015 http://www.who.int/hiv/data/en/
-
- Joint United Nations Programme on HIV/AIDS (UNAIDS) 90-90-90. An ambitious treatment target to help end the AIDS epidemic. Geneva: 2014. [accessed April 5, 2015]. http://www.unaids.org/sites/default/files/media_asset/90-90-90_en_0.pdf.
-
- Harries AD, Zachariah R, van Oosterhout JJ, et al. Diagnosis and management of antiretroviral-therapy failure in resource-limited settings in sub-Saharan Africa: challenges and perspectives. Lancet Infect Dis. 2010;10:60–65. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
