

Appropriate initial antibiotic therapy in hospitalized patients with gram-negative infections: systematic review and meta-analysis
- PMID: 26423743
- PMCID: PMC4589179
- DOI: 10.1186/s12879-015-1123-5
Appropriate initial antibiotic therapy in hospitalized patients with gram-negative infections: systematic review and meta-analysis
Abstract
Background: The rapid global spread of multi-resistant bacteria and loss of antibiotic effectiveness increases the risk of initial inappropriate antibiotic therapy (IAT) and poses a serious threat to patient safety. We conducted a systematic review and meta-analysis of published studies to summarize the effect of appropriate antibiotic therapy (AAT) or IAT against gram-negative bacterial infections in the hospital setting.
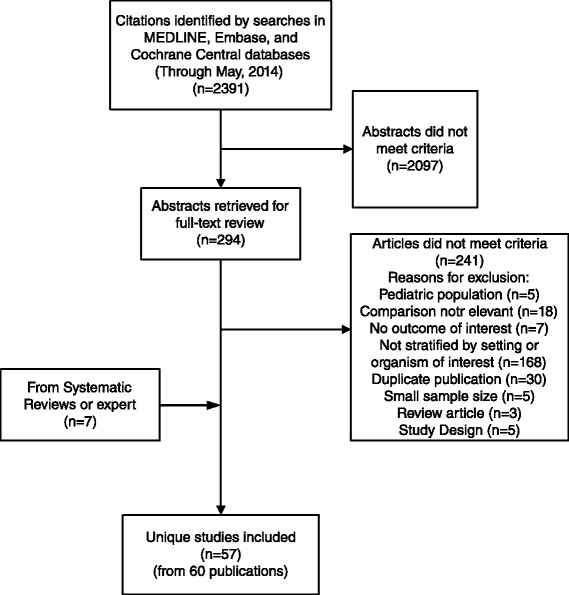
Methods: MEDLINE, EMBASE, and Cochrane CENTRAL databases were searched until May 2014 to identify English-language studies examining use of AAT or IAT in hospitalized patients with Gram-negative pathogens. Outcomes of interest included mortality, clinical cure, cost, and length of stay. Citations and eligible full-text articles were screened in duplicate. Random effect models meta-analysis was used.
Results: Fifty-seven studies in 60 publications were eligible. AAT was associated with lower risk of mortality (unadjusted summary odds ratio [OR] 0.38, 95 % confidence interval [CI] 0.30-0.47, 39 studies, 5809 patients) and treatment failure (OR 0.22, 95 % CI 0.14-0.35; 3 studies, 283 patients). Conversely, IAT increased risk of mortality (unadjusted summary OR 2.66, 95 % CI 2.12-3.35; 39 studies, 5809 patients). In meta-analyses of adjusted data, AAT was associated with lower risk of mortality (adjusted summary OR 0.43, 95 % CI 0.23-0.83; 6 studies, 1409 patients). Conversely, IAT increased risk of mortality (adjusted summary OR 3.30, 95 % CI 2.42-4.49; 16 studies, 2493 patients). A limited number of studies suggested higher cost and longer hospital stay with IAT. There was considerable heterogeneity in the definition of AAT or IAT, pathogens studied, and outcomes assessed.
Discussion: Using a large set of studies we found that IAT is associated with a number of serious consequences,including an increased risk of hospital mortality. Infections caused by drug-resistant, Gram-negative organisms represent a considerable financial burden to healthcare systems due to the increased costs associated with the resources required to manage the infection, particularly longer hospital stays. However, there were insufficient data that evaluated AAT for the outcome of costs among patients with nosocomialGram-negative infections.
Conclusions: IAT in hospitalized patients with Gram-negative infections is associated with adverse outcomes. Technological advances for rapid diagnostics to facilitate AAT along with antimicrobial stewardship, surveillance, infection control, and prevention is needed.
Figures




References
-
- Healthcare-associated Infections (HAIs). HAI Prevalence Data and Statistics. Centers for Disease Control and Prevention website. Available online: http://www.cdc.gov/HAI/surveillance/index.html. Accessed January 12, 2015
-
- Sievert DM, Ricks P, Edwards JR, Schneider A, Patel J, Srinivasan A, et al. Antimicrobial-resistant pathogens associated with healthcare-associated infections: summary of data reported to the national healthcare safety network at the centers for disease control and prevention, 2009–2010. Infect Control Hosp Epidemiol. 2013;34:1–14. doi: 10.1086/668770. - DOI - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
