

Idiopathic Pulmonary Fibrosis: Gender-Age-Physiology Index Stage for Predicting Future Lung Function Decline
- PMID: 26425858
- PMCID: PMC4944785
- DOI: 10.1378/chest.15-0530
Idiopathic Pulmonary Fibrosis: Gender-Age-Physiology Index Stage for Predicting Future Lung Function Decline
Abstract
Background: Idiopathic pulmonary fibrosis is a progressive lung disease with variable course. The Gender-Age-Physiology (GAP) Index and staging system uses clinical variables to stage mortality risk. It is unknown whether clinical staging predicts future decline in pulmonary function. We assessed whether the GAP stage predicts future pulmonary function decline and whether interval pulmonary function change predicts mortality after accounting for stage.
Methods: Patients with idiopathic pulmonary fibrosis (N = 657) were identified retrospectively at three tertiary referral centers, and baseline GAP stages were assessed. Mixed models were used to describe average trajectories of FVC and diffusing capacity of the lung for carbon monoxide (Dlco). Multivariable Cox proportional hazards models were used to assess whether declines in pulmonary function ≥ 10% in 6 months predict mortality after accounting for GAP stage.
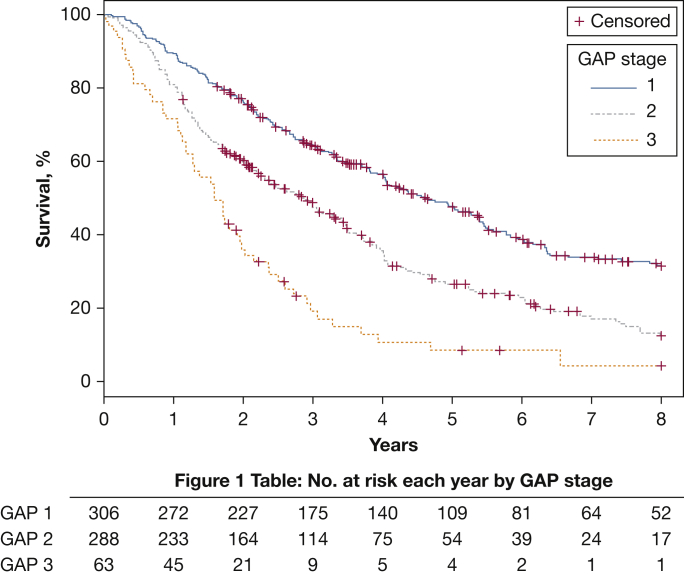
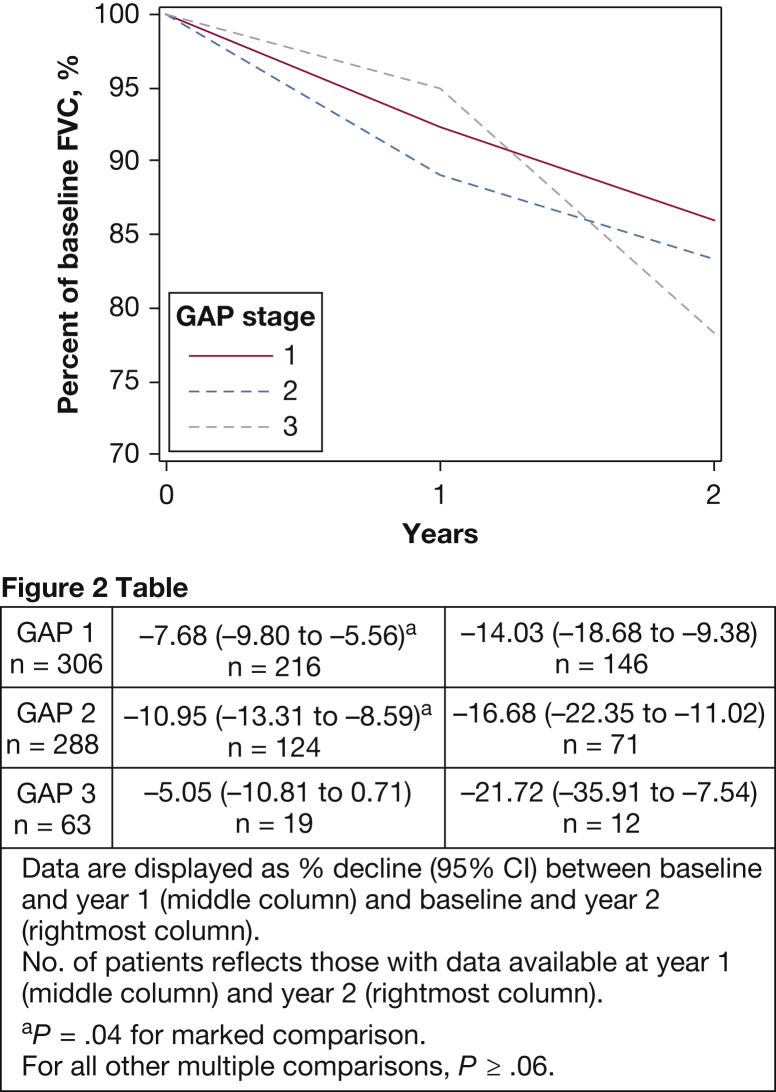
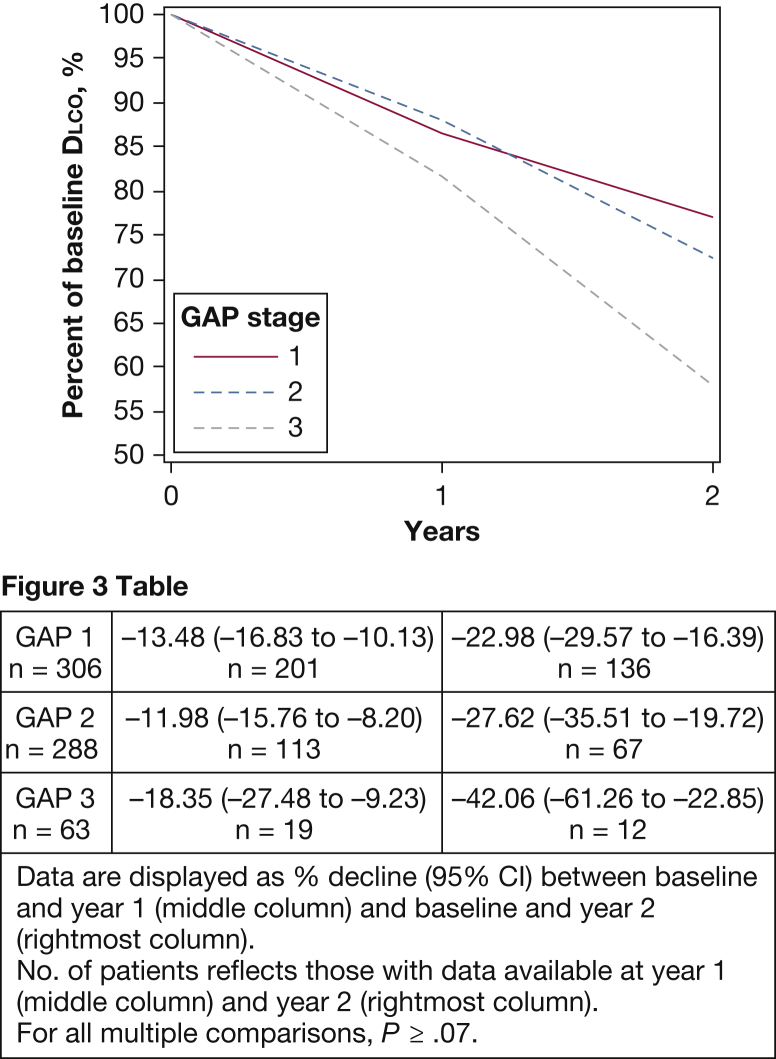
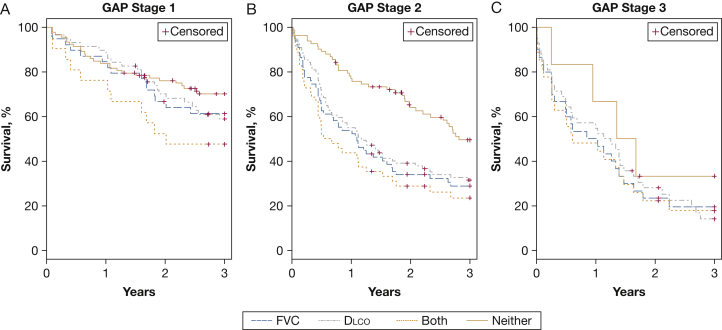
Results: Over a 2-year period, GAP stage was not associated with differences in yearly lung function decline. After accounting for stage, a 10% decrease in FVC or Dlco over 6 months independently predicted death or transplantation (FVC hazard ratio, 1.37; Dlco hazard ratio, 1.30; both, P ≤ .03). Patients with GAP stage 2 with declining pulmonary function experienced a survival profile similar to patients with GAP stage 3, with 1-year event-free survival of 59.3% (95% CI, 49.4-67.8) vs 56.9% (95% CI, 42.2-69.1).
Conclusions: Baseline GAP stage predicted death or lung transplantation but not the rate of future pulmonary function decline. After accounting for GAP stage, a decline of ≥ 10% over 6 months independently predicted death or lung transplantation.
Keywords: idiopathic pulmonary fibrosis; interstitial lung disease; lung function.
Copyright © 2016 American College of Chest Physicians. Published by Elsevier Inc. All rights reserved.
Figures
References
-
- Ley B., Collard H.R., King T.E., Jr. Clinical course and prediction of survival in idiopathic pulmonary fibrosis. Am J Respir Crit Care Med. 2011;183(4):431–440. - PubMed
-
- Collard H.R., King T.E., Jr., Bartelson B.B., Vourlekis J.S., Schwarz M.I., Brown K.K. Changes in clinical and physiologic variables predict survival in idiopathic pulmonary fibrosis. Am J Respir Crit Care Med. 2003;168(5):538–542. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
