

Timing of Estradiol Treatment After Menopause May Determine Benefit or Harm to Insulin Action
- PMID: 26425886
- PMCID: PMC4667161
- DOI: 10.1210/jc.2015-3084
Timing of Estradiol Treatment After Menopause May Determine Benefit or Harm to Insulin Action
Abstract
Context: Type 2 diabetes (T2D) is reduced in postmenopausal women randomized to estrogen-based hormone therapy (HT) compared with placebo. Insulin sensitivity is a key determinant of T2D risk and overall cardiometabolic health, and studies indicate that estradiol (E2) directly impacts insulin action.
Objective: We hypothesized that the timing of E2 administration after menopause is an important determinant of its effect on insulin action.
Design: We performed a randomized, crossover, placebo-controlled study.
Participants: Study participants were early postmenopausal (EPM; ≤ 6 years of final menses; n = 22) and late postmenopausal (LPM; ≥ 10 years since last menses; n = 24) women naive to HT.
Intervention: Study interventions included short-term (1 week) transdermal E2 and placebo.
Main outcomes and measures: The study's main outcome was insulin-mediated glucose disposal (glucose disposal rate [GDR]) via hyperinsulinemic-euglycemic clamp.
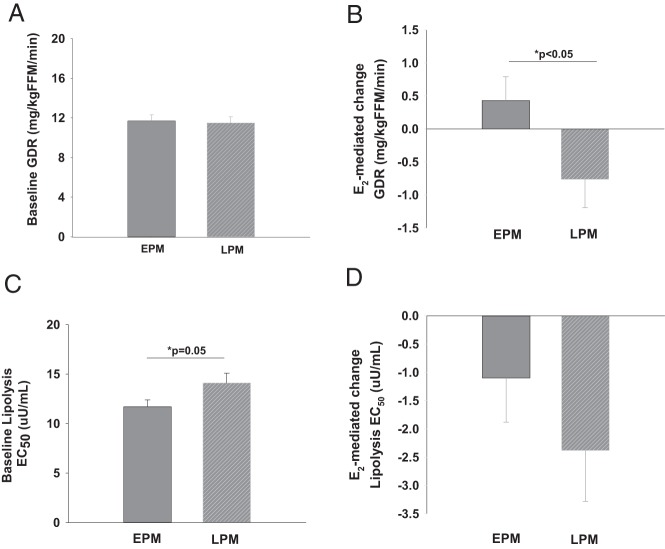
Results: Compared to EPM women, LPM women were older (mean ± SD; 63 ± 3 vs 56 ± 4 years, P < .05) and more years past menopause (12 ± 2 vs 3 ± 2 years, P < .05). Body mass index (24 ± 3 vs 25 ± 7 kg/m(2)) and fat mass (25 ± 7 vs 23 ± 6 kg) did not differ between groups, but fat-free mass (FFM) was lower in LPM women compared to EPM women (40 ± 4 vs 43 ± 5 kg, P < .05). Baseline GDR did not differ between groups (11.7 ± 2.8 vs 11.5 ± 2.9 mg/kg FFM/min). In support of our hypothesis, 1 week of E2 decreased GDR in LPM women compared to an increase in EPM women (+0.44 ± 1.7 vs - 0.76 ± 2.1 mg/kg FFM/min, P < .05).
Conclusions: There was not an apparent decline in GDR with age or time since menopause per se. However, E2 action on GDR was dependent on time since menopause, such that there was an apparent benefit early (≤ 6 years) compared to harm later (≥ 10 years) in menopause. E2-mediated effects on insulin action may be one mechanism by which HT reduces the incidence of T2D in early postmenopausal women.
Trial registration: ClinicalTrials.gov NCT01605071.
Figures
References
-
- Clarkson TB. Estrogen effects on arteries vary with stage of reproductive life and extent of subclinical atherosclerosis progression. Menopause. 2007;14:373–384. - PubMed
-
- Clarkson TB, Melendez GC, Appt SE. Timing hypothesis for postmenopausal hormone therapy: its origin, current status, and future. Menopause. 2013;20:342–353. - PubMed
-
- Grodstein F, Manson JE, Stampfer MJ. Hormone therapy and coronary heart disease: the role of time since menopause and age at hormone initiation. J Womens Health (Larchmt). 2006;15:35–44. - PubMed
-
- Salpeter SR, Walsh JM, Ormiston TM, Greyber E, Buckley NS, Salpeter EE. Meta-analysis: effect of hormone-replacement therapy on components of the metabolic syndrome in postmenopausal women. Diabetes Obes Metab. 2006;8:538–554. - PubMed
-
- Rossouw JE, Prentice RL, Manson JE, et al. Postmenopausal hormone therapy and risk of cardiovascular disease by age and years since menopause. JAMA. 2007;297:1465–1477. - PubMed
Publication types
MeSH terms
Substances
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
