

Prevalence and Predictors of Quality of Recovery at Home After Day Surgery
- PMID: 26426622
- PMCID: PMC4616829
- DOI: 10.1097/MD.0000000000001553
Prevalence and Predictors of Quality of Recovery at Home After Day Surgery
Abstract
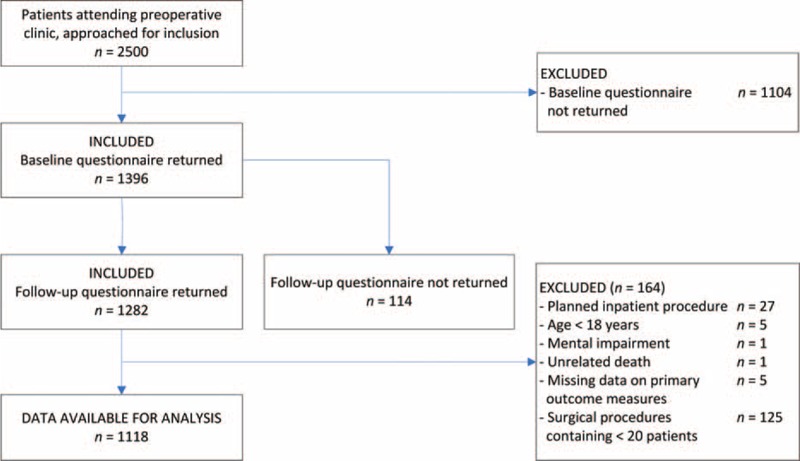
Traditionally, major complications and unanticipated admission/readmission rates were used to assess outcome after day surgery. However, in view of the relative absence of major complications the quality of recovery (QOR) should be considered one of the principal endpoints after day surgery. In our study, the level of QOR is defined by a combination of the Global Surgical Recovery (GSR) Index and the Quality of Life (QOL). The aim of this study was to analyze prevalence and predictors of QOR after day surgery on the fourth postoperative day. Elective patients scheduled for day surgery from November 2008 to April 2010 were enrolled in a prospective cohort study. Outcome parameters were measured by using questionnaire packages at 2 time points: 1 week preoperatively and 4 days postoperatively. Primary outcome parameter is the QOR and is defined as good if the GSR index >80% as well as the postoperative QOL is unchanged or improved as compared with baseline. QOR is defined as poor if both the GSR index ≤ 80% and if the postoperative QOL is decreased as compared with baseline. QOR is defined as intermediate in all other cases. Three logistic regression analyses were performed to determine predictors for poor QOR after day surgery. A total of 1118 patients were included. A good QOR was noted in 17.3% of patients, an intermediate QOR in 34.8%, and a poor QOR in 47.8% 4 days after day surgery. The best predictor for poor QOR after day surgery was type of surgery. Other predictors were younger age, work status, and longer duration of surgery. A history of previous surgery, expected pain (by the patient) and high long-term surgical fear were significant predictors of poor QOR in only 1 of 3 prediction models. The QOR at home 4 days after day surgery was poor in the majority of patients and showed a significant procedure-specific variation. Patients at risk for poor QOR can be identified during the preoperative period based on type of surgery, age, work status, and the duration of the surgery.
Conflict of interest statement
The authors have no funding and conflicts of interest to disclose.
Figures
References
-
- Cullen KA, Hall MJ, Golosinskiy A. Ambulatory surgery in the United States, 2006. Natl Health Stat Rep 2009; 11:1–25. - PubMed
-
- Chung F, Un V, Su J. Postoperative symptoms 24 hours after ambulatory anaesthesia. Can J Anaesth 1996; 43:1121–1127. - PubMed
-
- Fortier J, Chung F, Su J. Unanticipated admission after ambulatory surgery: a prospective study. Can J Anaesth 1998; 45:612–619. - PubMed
-
- Warner MA, Shields SE, Chute CG. Major morbidity and mortality within 1 month of ambulatory surgery and anesthesia. JAMA 1993; 270:1437–1441. - PubMed
-
- Mattila K, Hynynen M. Intensium Consortium Study G. Day surgery in Finland: a prospective cohort study of 14 day-surgery units. Acta Anaesthesiol Scand 2009; 53:455–463. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Miscellaneous
