

Association of Sodium Excretion With Metabolic Syndrome, Insulin Resistance, and Body Fat
- PMID: 26426658
- PMCID: PMC4616840
- DOI: 10.1097/MD.0000000000001650
Association of Sodium Excretion With Metabolic Syndrome, Insulin Resistance, and Body Fat
Abstract
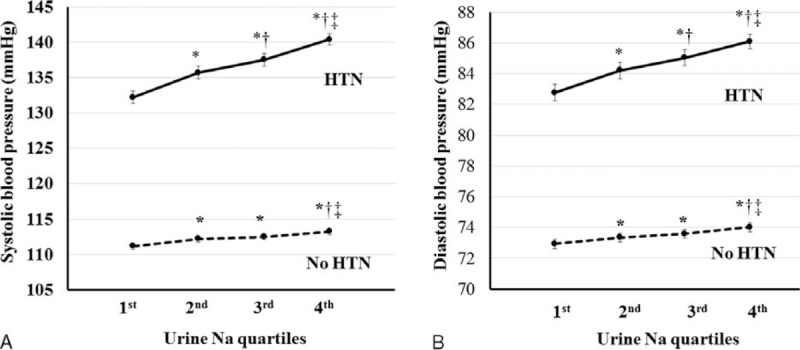
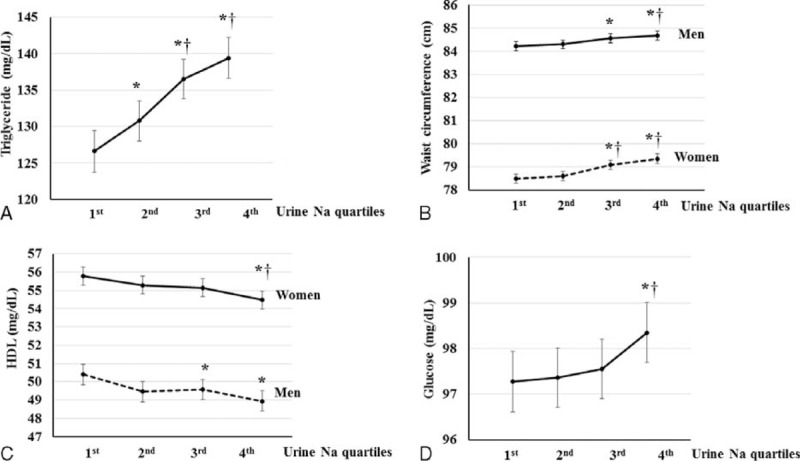
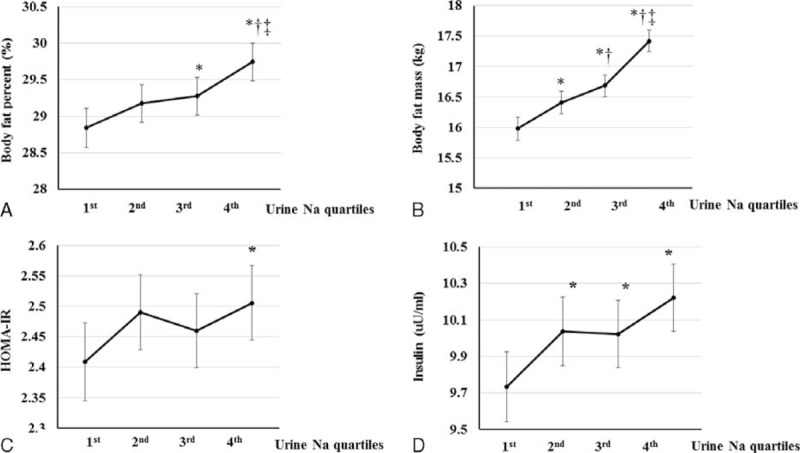
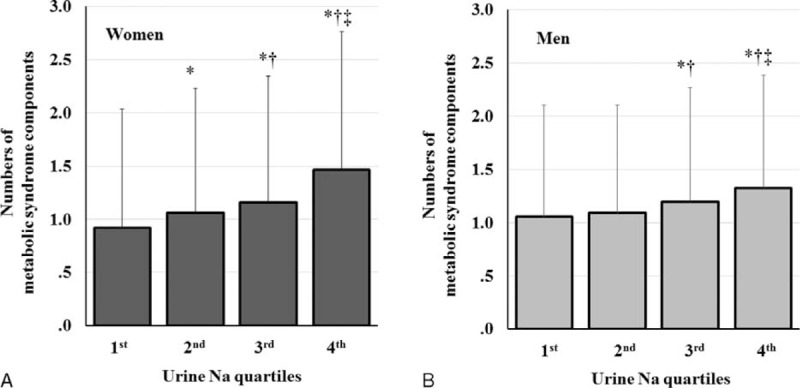
Sodium intake was reported to be related to metabolic syndrome (MS). Although a strong association between sodium intake and blood pressure (BP) has been reported, the relationship between sodium intake and other components of MS is unknown. An observational study of 18,146 adults in the Korea National Health and Nutrition Examination Survey IV-V databases (2008-2011) was performed. Estimates of 24-h sodium excretion were made from a single fasting urine sample. A significant positive association was found between sodium excretion and systolic BP and between sodium excretion and diastolic BP in participants with and without hypertension after adjusting for multiple covariates (P < 0.001 for trend). The relationship between triglyceride or glucose levels and sodium excretion was linear (P < 0.005). In both men and women, a positive relationship between sodium excretion and waist circumference and an inverse relationship between sodium excretion and high-density lipoprotein were found (P ≤ 0.001). Body fat percentage, body fat mass, and insulin level were positively related to sodium excretion (P ≤ 0.001), and HOMA-IR was significantly associated with sodium excretion (P < 0.05). The risk of MS was elevated 1.279-fold in the second quartile of sodium excretion (95% CI, 1.088-1.504, P = 0.003), 1.479-fold in the third quartile (95% CI, 1.262-1.734; P < 0.001), and 1.929-fold in the highest quartile (95% CI 1.654-2.249, P < .001) compared with the lowest quartile. Sodium intake is significantly associated with all components of MS, body fat, and insulin resistance. Therefore, a high-salt diet is a significant risk factor for MS.
Conflict of interest statement
The authors have no conflicts of interest to disclose.
Figures
References
-
- Mozaffarian D, Benjamin EJ, Go AS, et al. American Heart Association Statistics Committee and Stroke Statistics Subcommittee. Heart disease and stroke statistics-2015 update: a report from the American heart association. Circulation 2015; 131:e29–e322. - PubMed
-
- Ford ES. The metabolic syndrome and mortality from cardiovascular disease and all-causes: findings from the National Health and Nutrition Examination Survey II Mortality Study. Atherosclerosis 2004; 173:309–314. - PubMed
-
- Mottillo S, Filion KB, Genest J, et al. The metabolic syndrome and cardiovascular risk a systematic review and meta-analysis. J Am Coll Cardiol 2010; 56:1113–1132. - PubMed
-
- Hoffmann IS, Cubeddu LX. Salt and the metabolic syndrome. Nutr Metab Cardiovasc Dis 2009; 19:123–128. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
