

Incidences of Unfavorable Events in the Management of Low-Risk Papillary Microcarcinoma of the Thyroid by Active Surveillance Versus Immediate Surgery
- PMID: 26426735
- PMCID: PMC4739129
- DOI: 10.1089/thy.2015.0313
Incidences of Unfavorable Events in the Management of Low-Risk Papillary Microcarcinoma of the Thyroid by Active Surveillance Versus Immediate Surgery
Abstract
Background: The incidence of papillary microcarcinoma (PMC) of the thyroid is rapidly increasing globally, making the management of PMC an important clinical issue. Excellent oncological outcomes of active surveillance for low-risk PMC have been reported previously. Here, unfavorable events following active surveillance and surgical treatment for PMC were studied.
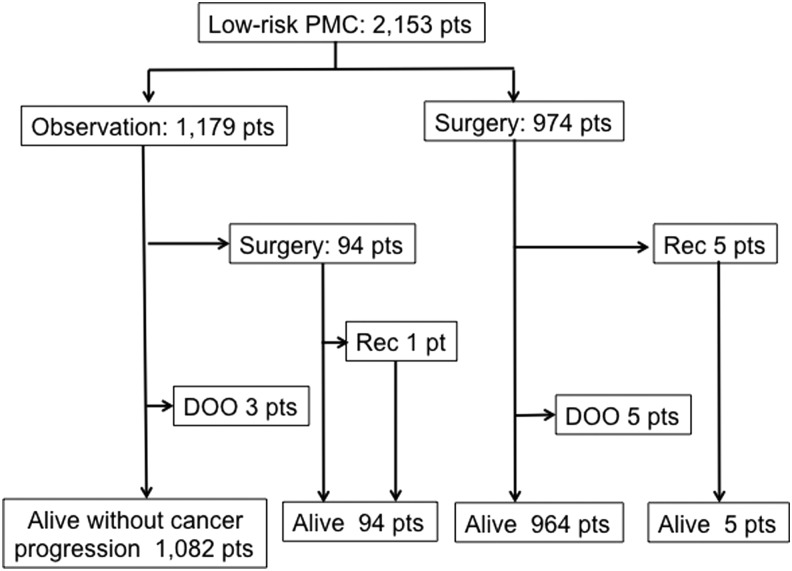
Methods: From February 2005 to August 2013, 2153 patients were diagnosed with low-risk PMC. Of these, 1179 patients chose active surveillance and 974 patients chose immediate surgery. The oncological outcomes and the incidences of unfavorable events of these groups were analyzed.
Results: In the active surveillance group, 94 patients underwent surgery for various reasons; tumor enlargement and the appearance of novel lymph node metastases were the reasons in 27 (2.3%) and six patients (0.5%), respectively. One of the patients with conversion to surgery had nodal recurrence, and five patients in the immediate surgery group had a recurrence in a cervical node or unresected thyroid lobe. All of these recurrences were successfully treated. None of the patients had distant metastases, and none died of the disease. The immediate surgery group had significantly higher incidences of transient vocal cord paralysis (VCP), transient hypoparathyroidism, and permanent hypoparathyroidism than the active-surveillance group did (4.1% vs. 0.6%, p < 0.0001; 16.7% vs. 2.8%, p < 0.0001; and 1.6% vs. 0.08%, p < 0.0001, respectively). Permanent VCP occurred only in two patients (0.2%) in the immediate surgery group. The proportion of patients on L-thyroxine for supplemental or thyrotropin (TSH)-suppressive purposes was significantly larger in the immediate surgery group than in the active surveillance group (66.1% vs. 20.7%, p < 0.0001). The immediate surgery group had significantly higher incidences of postsurgical hematoma and surgical scar in the neck compared with the active surveillance group (0.5% vs. 0%, p < 0.05; and 8.0% vs. 100%, p < 0.0001, respectively).
Conclusions: The oncological outcomes of the immediate surgery and active surveillance groups were similarly excellent, but the incidences of unfavorable events were definitely higher in the immediate surgery group. Thus, active surveillance is now recommended as the best choice for patients with low-risk PMC.
Figures
Comment in
-
[Active surveillance versus primary surgery for papillary microcarcinoma of the thyroid gland].Chirurg. 2017 Jan;88(1):71. doi: 10.1007/s00104-016-0331-x. Chirurg. 2017. PMID: 27928601 German. No abstract available.
References
-
- Davies L, Welch HG. 2014. Current thyroid cancer trends in the United States. JAMA Otolaryngol Head Neck Surg 140:317–322 - PubMed
-
- Sobin LH. 1990. Histological typing of thyroid tumours. Histopathology 16:513. - PubMed
-
- Ahn HS, Kim HJ, Welch HG. 2014. Korea's thyroid-cancer “epidemic”—screening and overdiagnosis. N Engl J Med 371:1765–1767 - PubMed
-
- Takebe K, Date M, Yamamoto Y. 1994. Mass screening for thyroid cancer with ultrasonography. KARKINOS 7:309–317[in Japanese]
-
- Harach HR, Franssila KO, Wasenius VM. 1985. Occult papillary carcinoma of the thyroid. A “normal” finding in Finland. A systematic autopsy study. Cancer 56:531–538 - PubMed
Publication types
MeSH terms
Supplementary concepts
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
