

Cesarean delivery is not associated with decreased at-birth fracture rates in osteogenesis imperfecta
- PMID: 26426884
- PMCID: PMC4818203
- DOI: 10.1038/gim.2015.131
Cesarean delivery is not associated with decreased at-birth fracture rates in osteogenesis imperfecta
Abstract
Purpose: Osteogenesis imperfecta (OI) predisposes to recurrent fractures. Patients with the moderate to severe forms of OI present with antenatal fractures, and the mode of delivery that would be safest for the fetus is not known.
Methods: We conducted systematic analyses of the largest cohort of individuals with OI (n = 540) enrolled to date in the OI Linked Clinical Research Centers. Self-reported at-birth fracture rates were compared among individuals with OI types I, III, and IV. Multivariate analyses utilizing backward-elimination logistic regression model building were performed to assess the effect of multiple covariates, including method of delivery, on fracture-related outcomes.
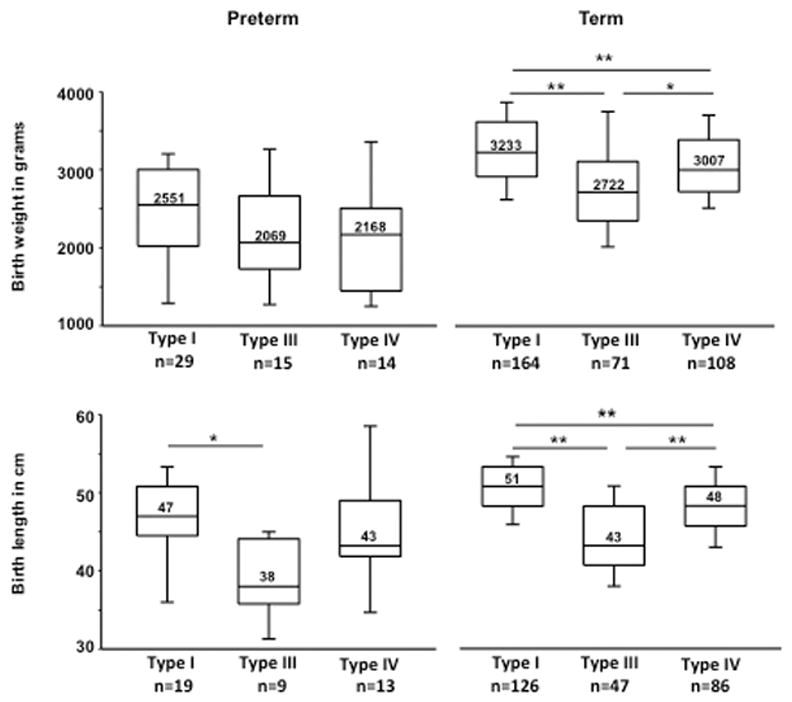
Results: When accounting for other covariates, at-birth fracture rates did not differ based on whether delivery was by vaginal route or by cesarean delivery (CD). Increased birth weight conferred higher risk for fractures irrespective of the delivery method. In utero fracture, maternal history of OI, and breech presentation were strong predictors for choosing CD.
Conclusion: Our study, the largest to analyze the effect of various factors on at-birth fracture rates in OI, shows that CD is not associated with decreased fracture rate. With the limitation that the fracture data were self-reported in this cohort, these results suggest that CD should be performed only for other maternal or fetal indications, not for the sole purpose of fracture prevention in OI.Genet Med 18 6, 570-576.
Figures
References
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
