

The placenta is the center of the chronic disease universe
- PMID: 26428494
- PMCID: PMC4593619
- DOI: 10.1016/j.ajog.2015.08.030
The placenta is the center of the chronic disease universe
Abstract
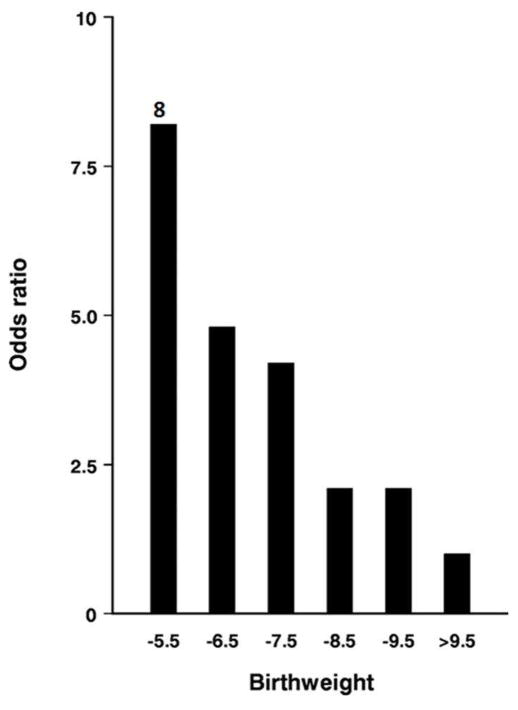
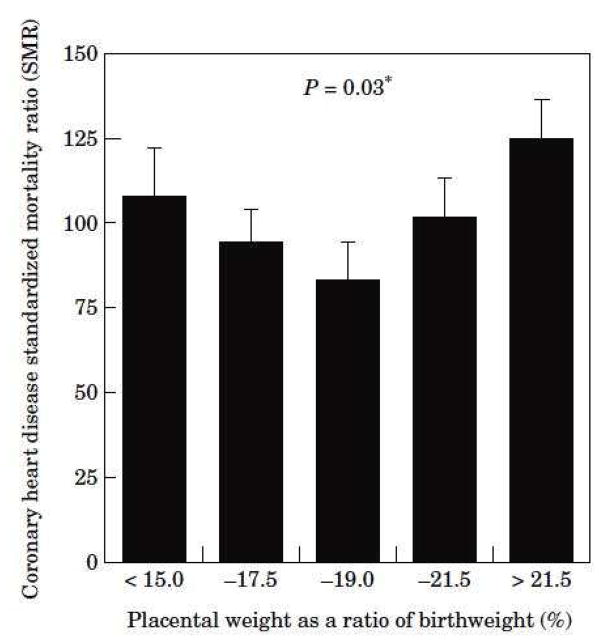
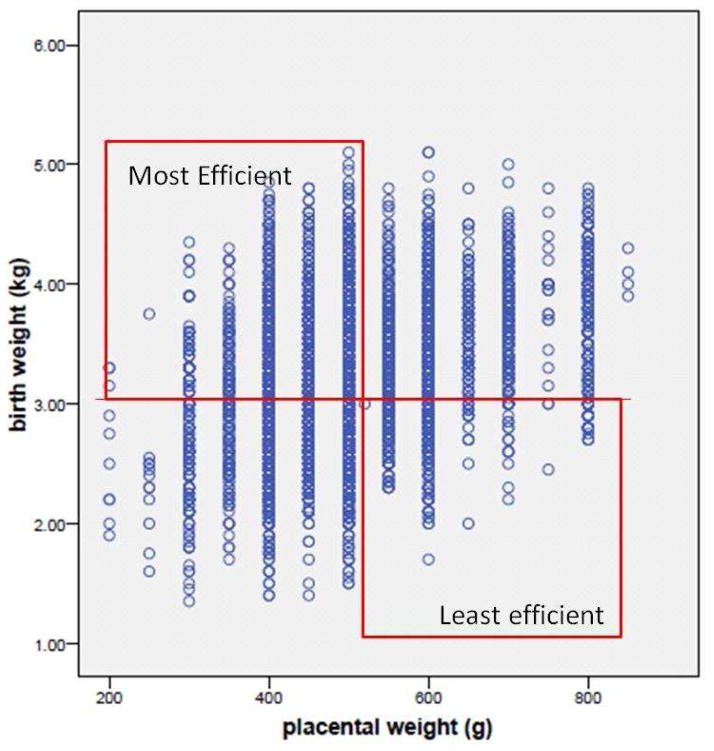
Over the past quarter century it has become clear that adult onset chronic diseases like heart disease and type 2 diabetes have their roots in early development. The report by David Barker and colleagues showing an inverse relationship between birthweight and mortality from ischemic heart disease was the first clear-cut demonstration of fetal programming. Because fetal growth depends upon the placental capacity to transport nutrients from maternal blood, it has been a suspected causative agent since the original Barker reports. Epidemiological studies have shown that placental size and shape have powerful associations with offspring disease. More recent studies have shown that maternal phenotypic characteristics, such as body mass index and height, interact with placental size and shape to predict disease with much more precision than does birthweight alone. For example, among people in the Helsinki Birth Cohort, who were born during 1924–1944, the risk for acquiring colorectal cancer increased as the placental surface became longer and more oval. Among people in whom the difference between the length and breadth of the surface exceeded 6 cm, the hazard ratio for the cancer was 2.3 (95% CI 1.2–4.7, p=0.003) compared with those in whom there was no difference. Among Finnish men, the hazard ratio for coronary heart disease was 1.07 (1.02–1.13, P =0.01) per 1% increase in the placental weight/birthweight ratio. Thus, it appears that the ratio of birthweight to placental weight, known as placental efficiency, predicts cardiovascular risk as well. Babies born with placentas at the extremes of efficiency are more vulnerable for adult onset chronic diseases. Recent evidence suggests that placental growth patterns are sex specific. Boys’ placentas are, in general, more efficient than those made by girls. Another recent discovery is that the size, shape and efficiencies of the placenta can change over years of time with very narrow confidence limits. This suggests that the growth of the placenta within a population of women is strongly affected by their nutritional environment. Even though it is known that an individual placenta can expand to improve its nutrient acquisition capacity in the first 2/3rd of gestation, the mechanisms by which placentas grow in response to a specific nutritional environment are not known. Discovering those mechanisms is the task of the current generation of scientists. While it may seem obvious that good nutrition is highly important for women who are pregnant because it supports optimal placentation and fetal development, more research is needed to determine the mechanisms by which maternal nutrition, placenta growth and fetal health are related.
Figures
References
-
- Plagemann A, Harder T, Dudenhausen JW. The diabetic pregnancy, macrosomia, and perinatal nutritional programming. Nestle Nutrition workshop series. Paediatric programme. 2008;61:91–102. - PubMed
-
- Oken E, Gillman MW. Fetal origins of obesity. Obesity research. 2003 Apr;11(4):496–506. - PubMed
-
- Wei JN, Sung FC, Li CY, et al. Low birth weight and high birth weight infants are both at an increased risk to have type 2 diabetes among schoolchildren in taiwan. Diabetes care. 2003 Feb;26(2):343–348. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
