

Chronic inflammation of the placenta: definition, classification, pathogenesis, and clinical significance
- PMID: 26428503
- PMCID: PMC4782598
- DOI: 10.1016/j.ajog.2015.08.041
Chronic inflammation of the placenta: definition, classification, pathogenesis, and clinical significance
Abstract
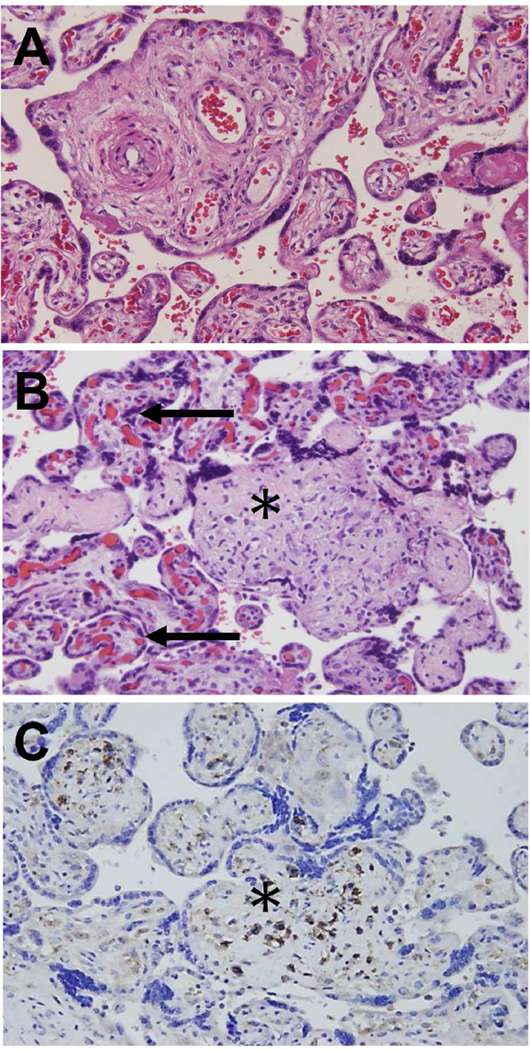
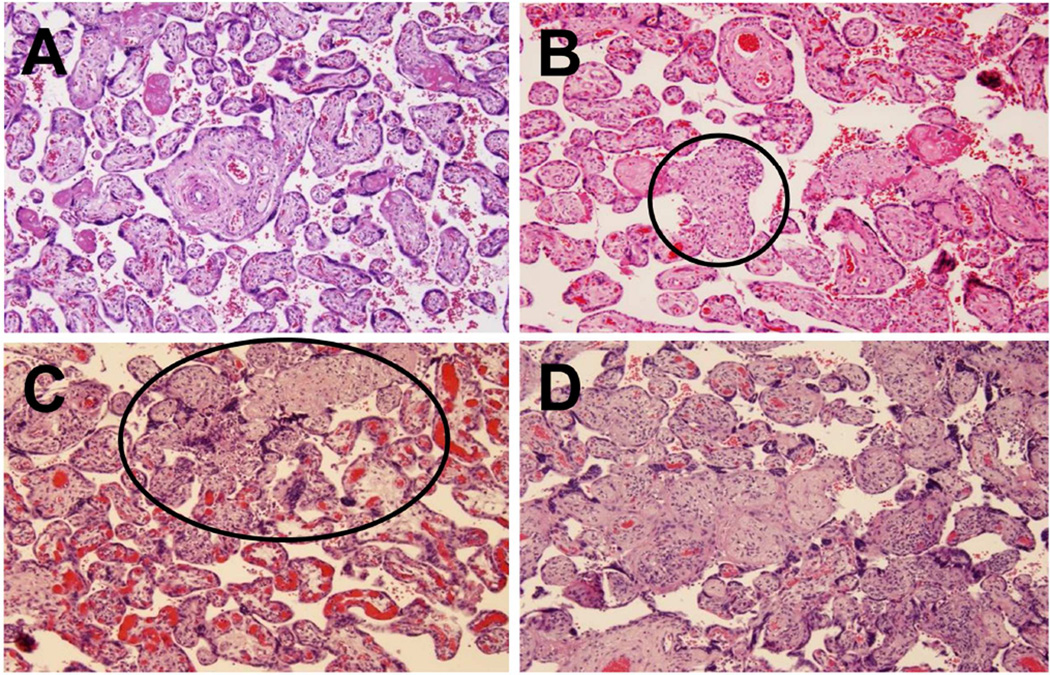
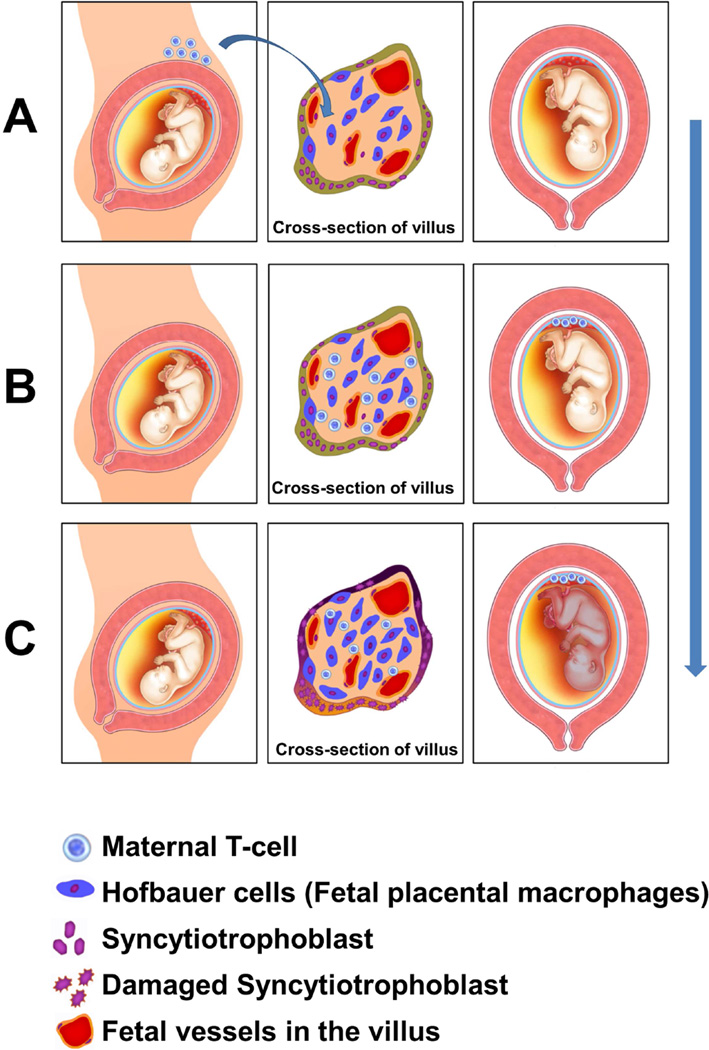
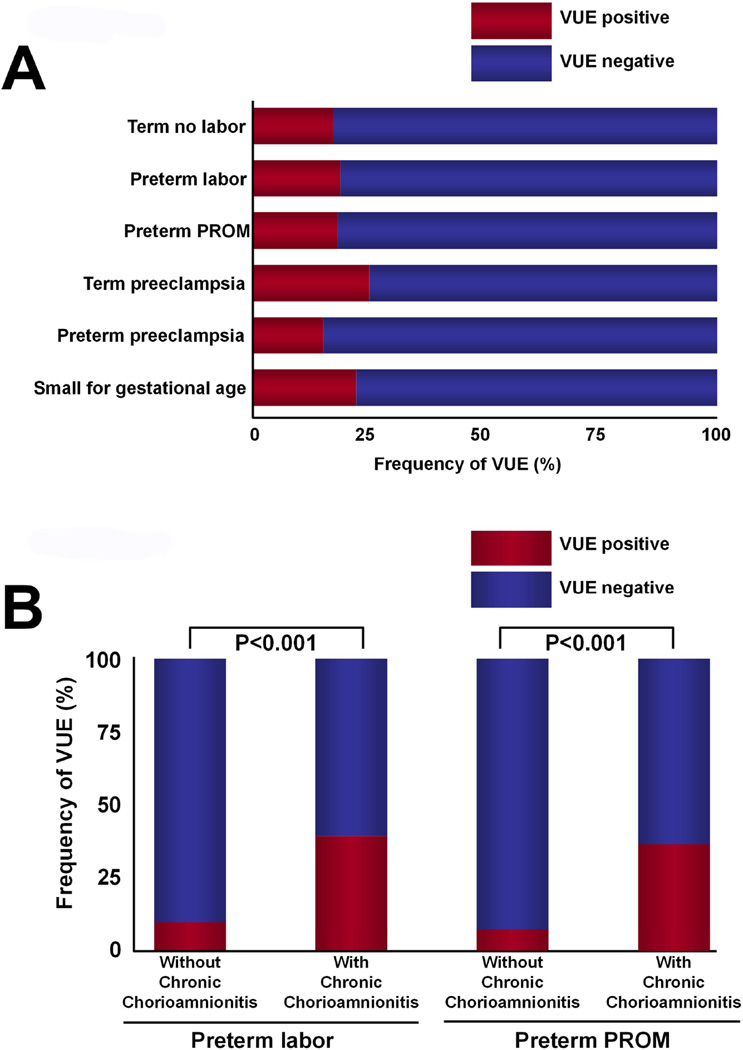
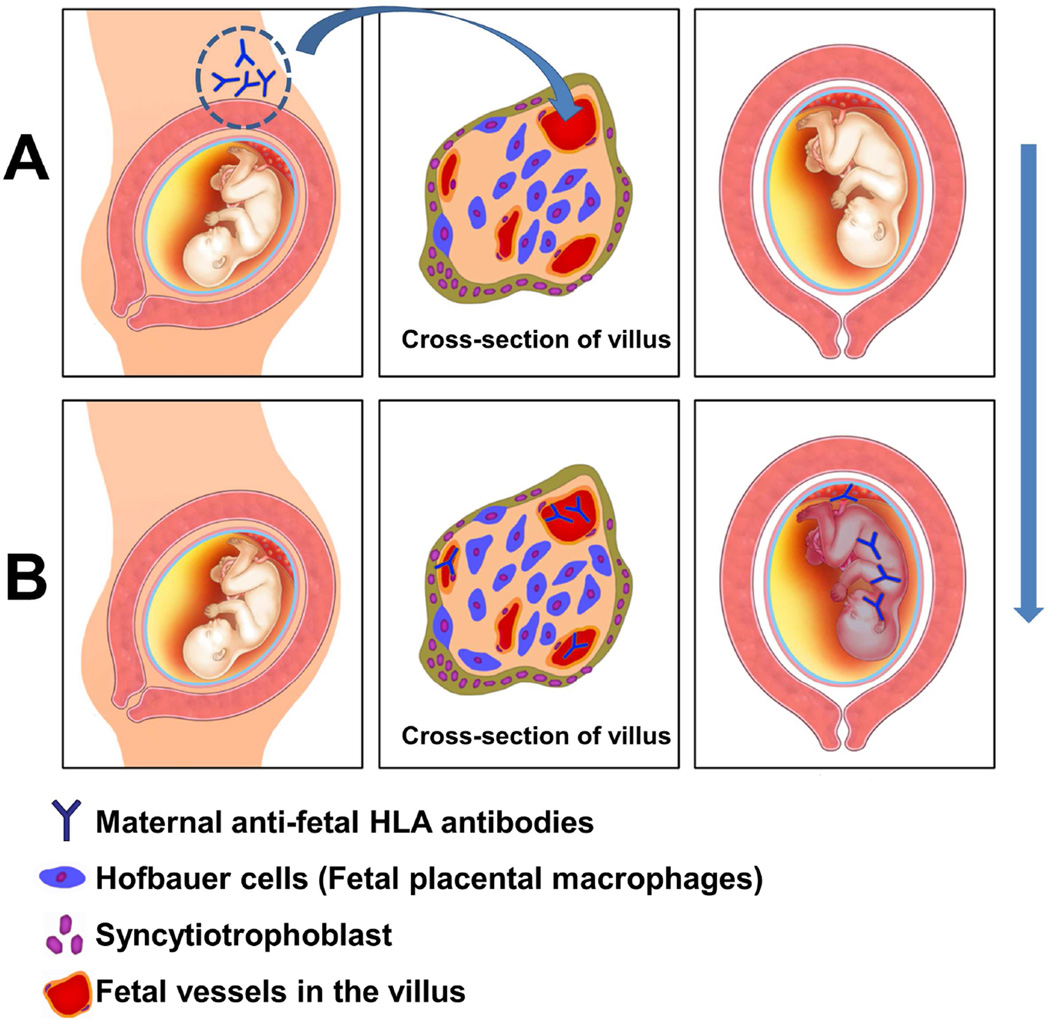
Chronic inflammatory lesions of the placenta are characterized by the infiltration of the organ by lymphocytes, plasma cells, and/or macrophages and may result from infections (viral, bacterial, parasitic) or be of immune origin (maternal anti-fetal rejection). The 3 major lesions are villitis (when the inflammatory process affects the villous tree), chronic chorioamnionitis (which affects the chorioamniotic membranes), and chronic deciduitis (which involves the decidua basalis). Maternal cellular infiltration is a common feature of the lesions. Villitis of unknown etiology (VUE) is a destructive villous inflammatory lesion that is characterized by the infiltration of maternal T cells (CD8+ cytotoxic T cells) into chorionic villi. Migration of maternal T cells into the villi is driven by the production of T-cell chemokines in the affected villi. Activation of macrophages in the villi has been implicated in the destruction of the villous architecture. VUE has been reported in association with preterm and term fetal growth restriction, preeclampsia, fetal death, and preterm labor. Infants whose placentas have VUE are at risk for death and abnormal neurodevelopmental outcome at the age of 2 years. Chronic chorioamnionitis is the most common lesion in late spontaneous preterm birth and is characterized by the infiltration of maternal CD8+ T cells into the chorioamniotic membranes. These cytotoxic T cells can induce trophoblast apoptosis and damage the fetal membranes. The lesion frequently is accompanied by VUE. Chronic deciduitis consists of the presence of lymphocytes or plasma cells in the basal plate of the placenta. This lesion is more common in pregnancies that result from egg donation and has been reported in a subset of patients with premature labor. Chronic placental inflammatory lesions can be due to maternal anti-fetal rejection, a process associated with the development of a novel form of fetal systemic inflammatory response. The syndrome is characterized by an elevation of the fetal plasma T-cell chemokine. The evidence that maternal anti-fetal rejection underlies the pathogenesis of many chronic inflammatory lesions of the placenta is reviewed. This article includes figures and histologic examples of all chronic inflammatory lesions of the placenta.
Keywords: C4d; CD8; CXCL10; HLA; T cell; VUE; allograft; chemokine; chronic chorioamnionitis; chronic deciduitis; complement; fetal death; fetal growth restriction; maternal floor infarction; plasma cells; prematurity; rejection; tolerance.
Published by Elsevier Inc.
Figures








References
-
- Murphy HS. Inflammation. In: Strayer DS, Rubin E, editors. Rubin’s Pathology. Sixth ed. China: Lippincott Williams & Wilkins; 2012. pp. 47–82.
-
- Benirschke K, Burton GJ, Baergen RN. Pathology of the Human Placenta. Sixth ed. Berlin Heidelberg: Springer; 2012. Infectious Diseases; pp. 557–656.
-
- Fox H, Sebire NJ. Pathology of the Placenta. Third ed. China: ELSEVIER; 2007. Infections and Inflammatory Lesions of the Placenta; pp. 303–354.
-
- Katzman PJ. Chronic inflammatory lesions of the placenta. Semin Perinatol. 2015;39(1):20–26. - PubMed
-
- Altshuler G, Russell P. The human placental villitides: a review of chronic intrauterine infection. Curr Top Pathol. 1975;60:64–112. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials
