

Usual Blood Pressure and Risk of New-Onset Diabetes: Evidence From 4.1 Million Adults and a Meta-Analysis of Prospective Studies
- PMID: 26429079
- PMCID: PMC4595710
- DOI: 10.1016/j.jacc.2015.07.059
Usual Blood Pressure and Risk of New-Onset Diabetes: Evidence From 4.1 Million Adults and a Meta-Analysis of Prospective Studies
Abstract
Background: Reliable quantification of the association between blood pressure (BP) and risk of type 2 diabetes is lacking.
Objectives: This study sought to determine the association between usual BP and risk of diabetes, overall and by participant characteristics.
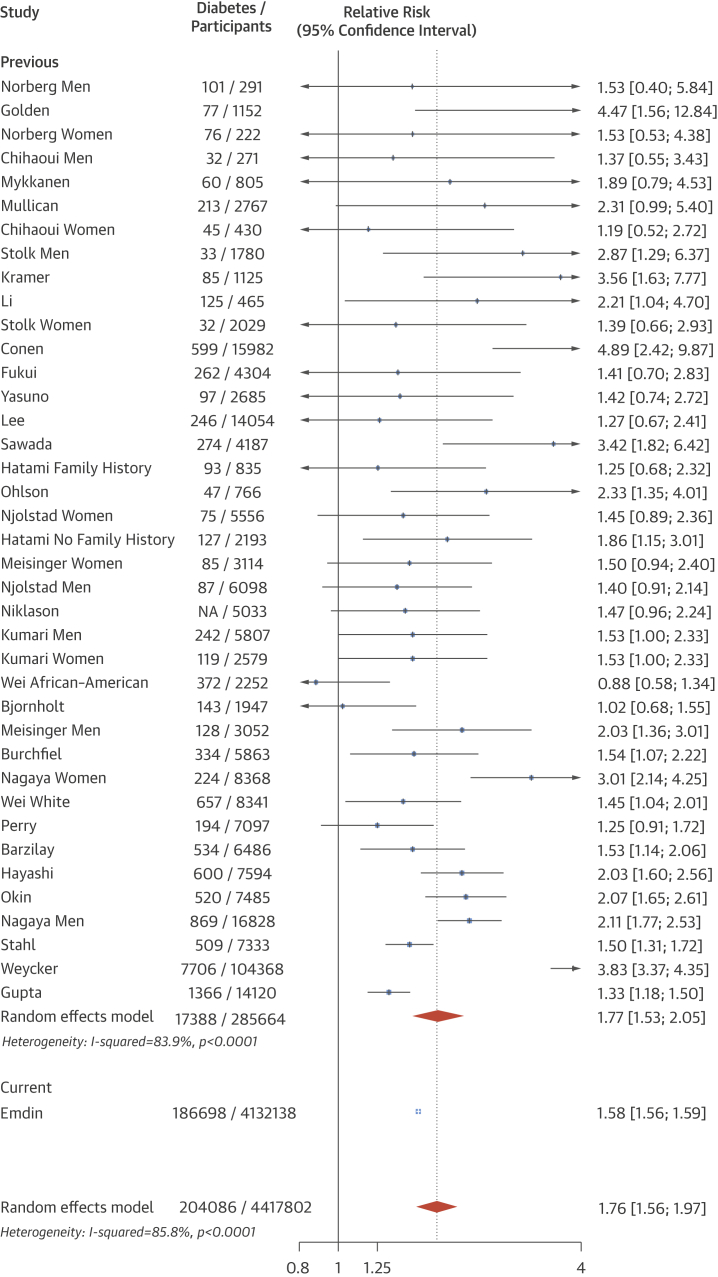
Methods: A cohort of 4.1 million adults, free of diabetes and cardiovascular disease, was identified using validated linked electronic health records. Analyses were complemented by a meta-analysis of prospective studies that reported relative risks of new-onset diabetes per unit of systolic blood pressure (SBP).
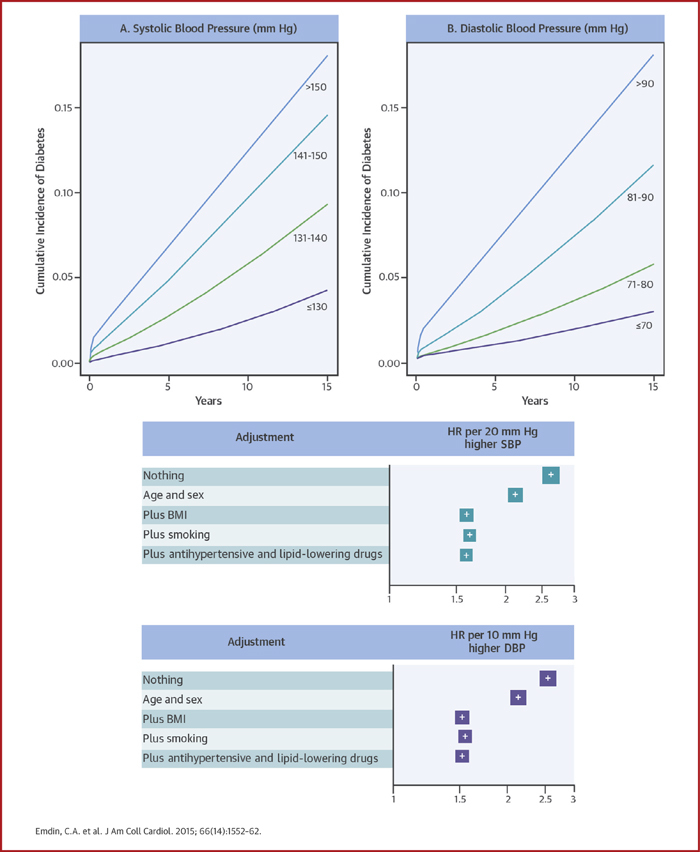
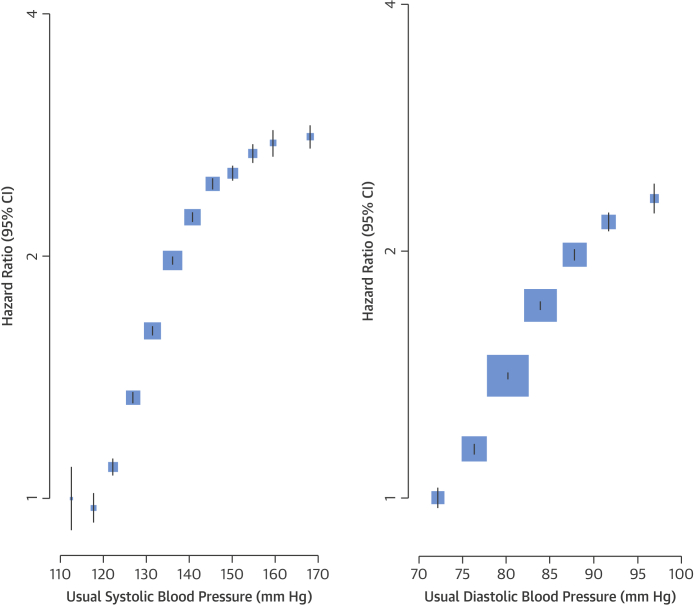
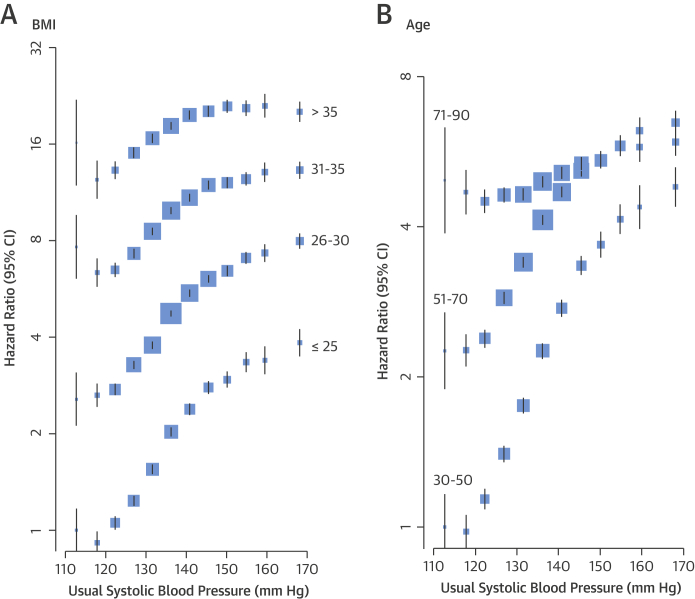
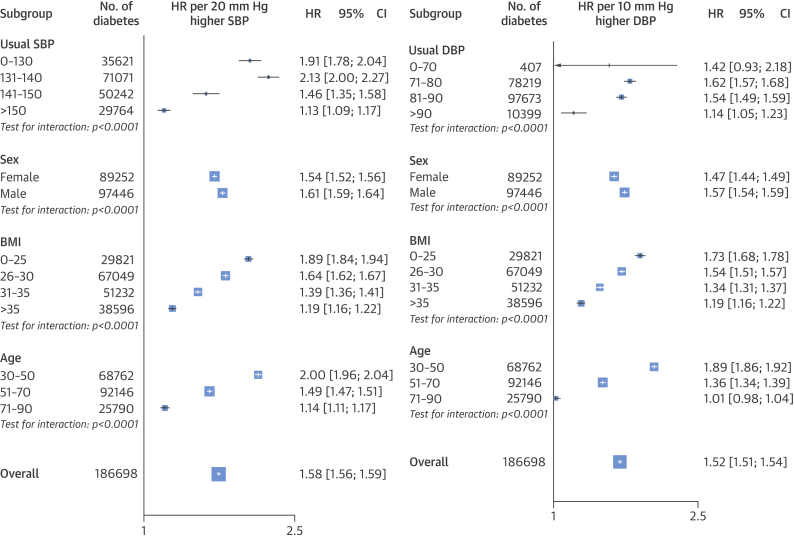
Results: Among the overall cohort, 20 mm Hg higher SBP and 10 mm Hg higher diastolic BP were associated with a 58% and a 52% higher risk of new-onset diabetes (hazard ratio: 1.58; 95% confidence interval [CI]: 1.56 to 1.59; and hazard ratio: 1.52; 95% confidence interval: 1.51 to 1.54), respectively. There was no evidence of a nadir to a baseline BP of 110/70 mm Hg. The strength of the association per 20 mm Hg higher SBP declined with age and with increasing body mass index. Estimates were similar even after excluding individuals prescribed antihypertensive or lipid-lowering therapies. Systematic review identified 30 studies with 285,664 participants and 17,388 incident diabetes events. The pooled relative risk of diabetes for a 20 mm Hg higher usual SBP across these studies was 1.77 (1.53 to 2.05).
Conclusions: People with elevated BP are at increased risk of diabetes. The strength of the association declined with increasing body mass index and age. Further research should determine if the observed risk is modifiable.
Keywords: body mass index; meta-analysis; regression dilution bias.
Copyright © 2015 American College of Cardiology Foundation. Published by Elsevier Inc. All rights reserved.
Figures
Comment in
-
High blood pressure is linked to increased risk of diabetes.BMJ. 2015 Sep 29;351:h5167. doi: 10.1136/bmj.h5167. BMJ. 2015. PMID: 26424006 No abstract available.
-
Analysis of Large Electronic Health Record Databases Supports Blood Pressure-Incident Diabetes Association.J Am Coll Cardiol. 2015 Oct 6;66(14):1563-1565. doi: 10.1016/j.jacc.2015.07.058. J Am Coll Cardiol. 2015. PMID: 26429080 No abstract available.
-
Usual Blood Pressure and New-Onset Diabetes Risk: Evidence From 4.1 Million Adults and a Meta-Analysis.J Am Coll Cardiol. 2016 Apr 5;67(13):1656-1657. doi: 10.1016/j.jacc.2015.12.065. J Am Coll Cardiol. 2016. PMID: 27150694 No abstract available.
References
-
- Whiting D.R., Guariguata L., Weil C., Shaw J. IDF diabetes atlas: global estimates of the prevalence of diabetes for 2011 and 2030. Diabetes Res Clin Pract. 2011;94:311–321. - PubMed
-
- Kannel W.B., McGee D.L. Diabetes and cardiovascular risk factors: the Framingham study. Circulation. 1979;59:8–13. - PubMed
-
- Lewington S., Clarke R., Qizilbash N., Peto R., Collins R., Prospective Studies Collaboration Age-specific relevance of usual blood pressure to vascular mortality: a meta-analysis of individual data for one million adults in 61 prospective studies. Lancet. 2002;360:1903–1913. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
