

Risk Stratification for Rejection and Infection after Kidney Transplantation
- PMID: 26430088
- PMCID: PMC4670759
- DOI: 10.2215/CJN.01790215
Risk Stratification for Rejection and Infection after Kidney Transplantation
Abstract
Background and objectives: Definition of individual risk profile is the first step to implement strategies to keep the delicate balance between under- and overimmunosuppression after kidney transplantation.
Design, setting, participants, & measurements: We used data from the Efficacy Limiting Toxicity Elimination Symphony Study (1190 patients between 2002 and 2004) to model risk of rejection and infection in the first year after kidney transplantation. External validation was performed in a study population from the Fixed-Dose Concentration-Controlled Trial (630 patients between 2003 and 2006).
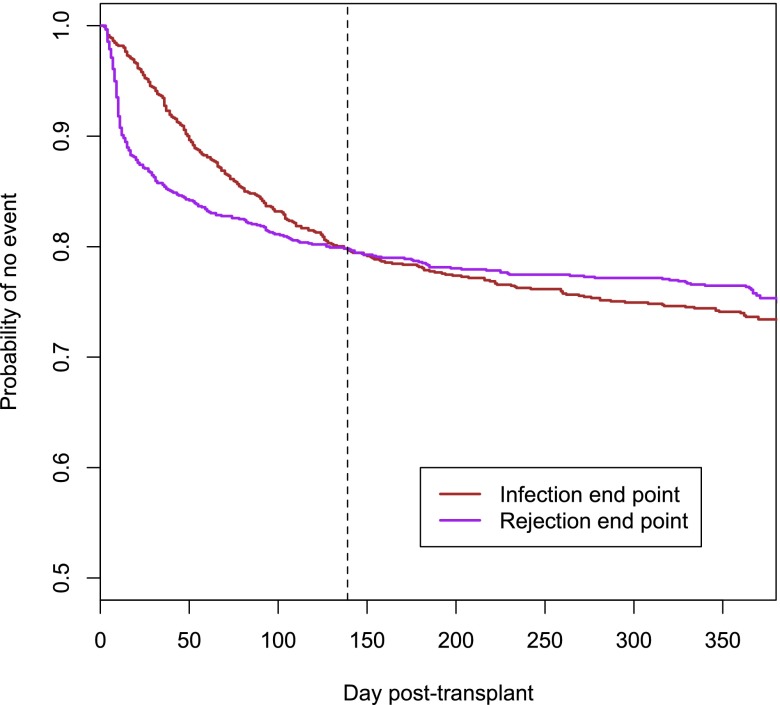
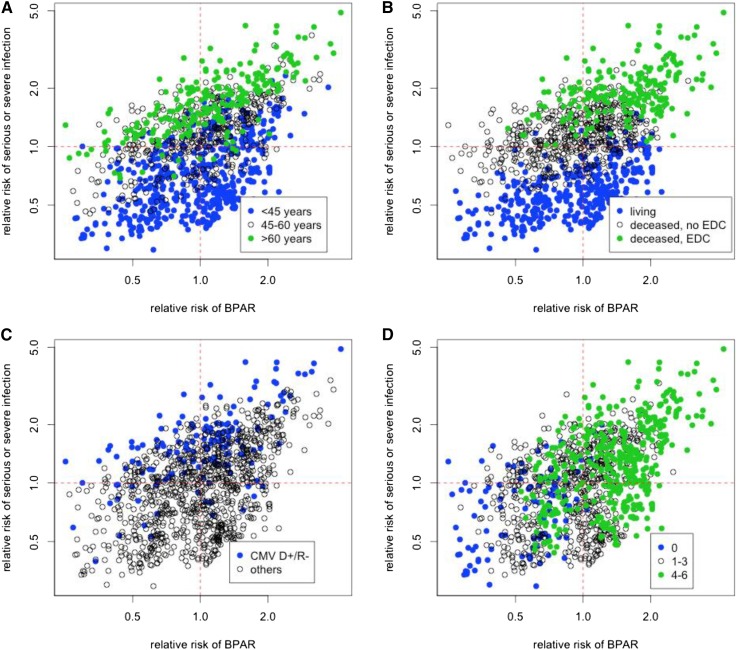
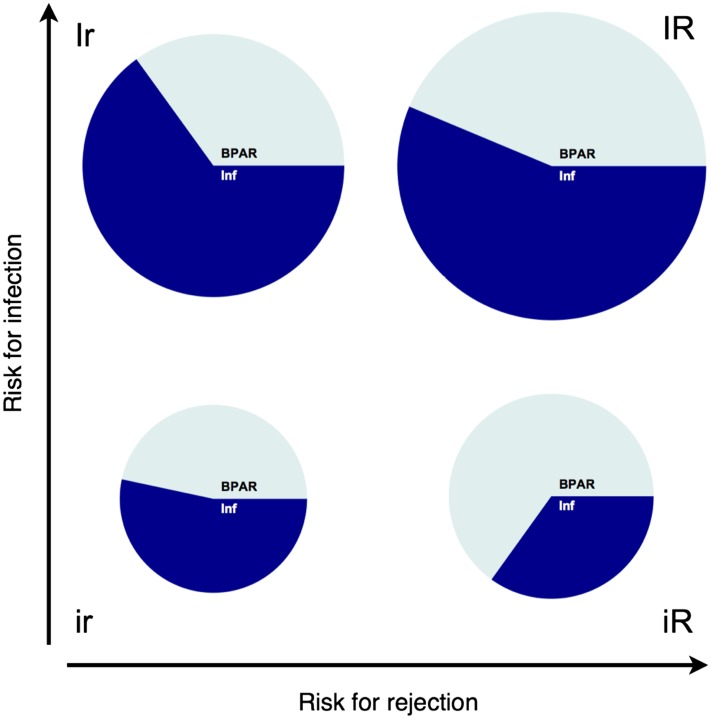
Results: Despite different temporal dynamics, rejections and severe infections had similar overall incidences in the first year after transplantation (23.4% and 25.5%, respectively), and infections were the principal cause of death (43.2% of all deaths). Recipient older age, deceased donor, higher number of HLA mismatches, and high risk for cytomegalovirus disease were associated with infection; deceased donor, higher number of HLA mismatches, and immunosuppressive therapy including cyclosporin A (compared with tacrolimus), with rejection. These factors were integrated into a two-dimensional risk stratification model, which defined four risk groups: low risk for infection and rejection (30.8%), isolated risk for rejection (36.1%), isolated risk for infection (7.0%), and high risk for infection and rejection (26.1%). In internal validation, this model significantly discriminated the subgroups in terms of composite end point (low risk for infection/rejection, 24.4%; isolated risk for rejection and isolated risk for infection, 31.3%; high risk for infection/rejection, 54.4%; P<0.001), rejection episodes (isolated risk for infection and low risk for infection/rejection, 13.0%; isolated risk for rejection and high risk for infection/rejection, 24.2%; P=0.001), and infection episodes (low risk for infection/rejection and isolated risk for rejection, 12.0%; isolated risk for infection and high risk for infection/rejection, 37.6%; P<0.001). External validation confirmed the applicability of the model to an independent cohort.
Conclusions: We propose a two-dimensional risk stratification model able to disentangle the individual risk for rejection and infection in the first year after kidney transplantation. This concept can be applied to implement a personalized immunosuppressive and antimicrobial treatment approach.
Keywords: cause of death; cyclosporin; death; humans; immunosuppression; kidney transplantation; tacrolimus; transplant infectious disease; transplant outcomes; transplant recipients.
Copyright © 2015 by the American Society of Nephrology.
Figures
References
-
- Sayegh MH, Carpenter CB: Transplantation 50 years later--progress, challenges, and promises. N Engl J Med 351: 2761–2766, 2004 - PubMed
-
- Pascual M, Theruvath T, Kawai T, Tolkoff-Rubin N, Cosimi AB: Strategies to improve long-term outcomes after renal transplantation. N Engl J Med 346: 580–590, 2002 - PubMed
-
- Fishman JA, Issa NC: Infection in organ transplantation: Risk factors and evolving patterns of infection. Infect Dis Clin North Am 24: 273–283, 2010 - PubMed
-
- Karuthu S, Blumberg EA: Common infections in kidney transplant recipients. Clin J Am Soc Nephrol 7: 2058–2070, 2012 - PubMed
-
- Fishman JA: Infection in solid-organ transplant recipients. N Engl J Med 357: 2601–2614, 2007 - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
