

Minocycline potentiates the anti-hyperalgesic effect of ceftriaxone in CCI-induced neuropathic pain in rats
- PMID: 26430455
- PMCID: PMC4578210
Minocycline potentiates the anti-hyperalgesic effect of ceftriaxone in CCI-induced neuropathic pain in rats
Abstract
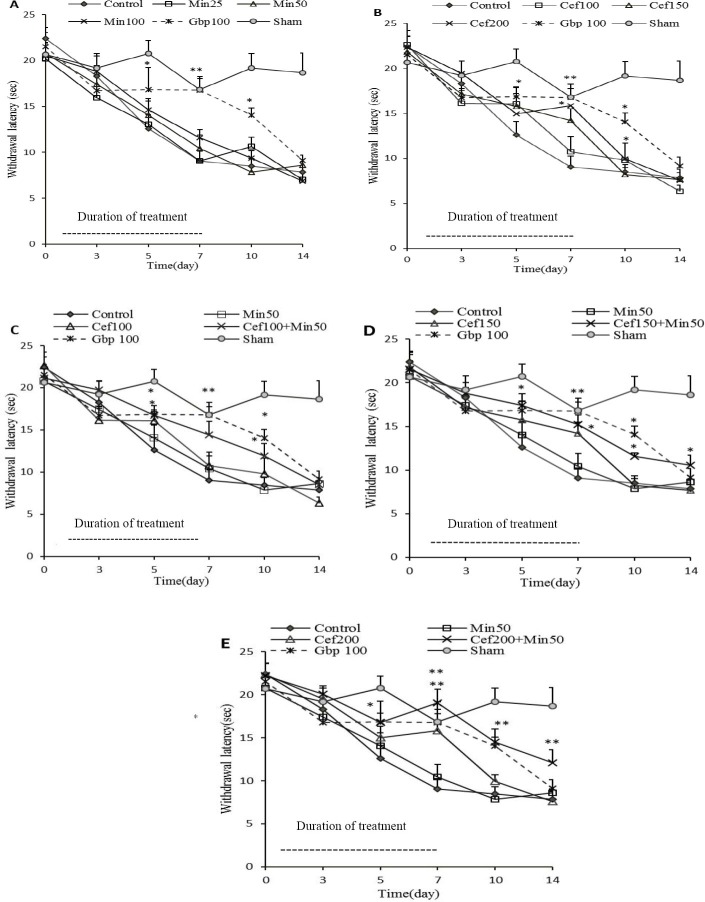
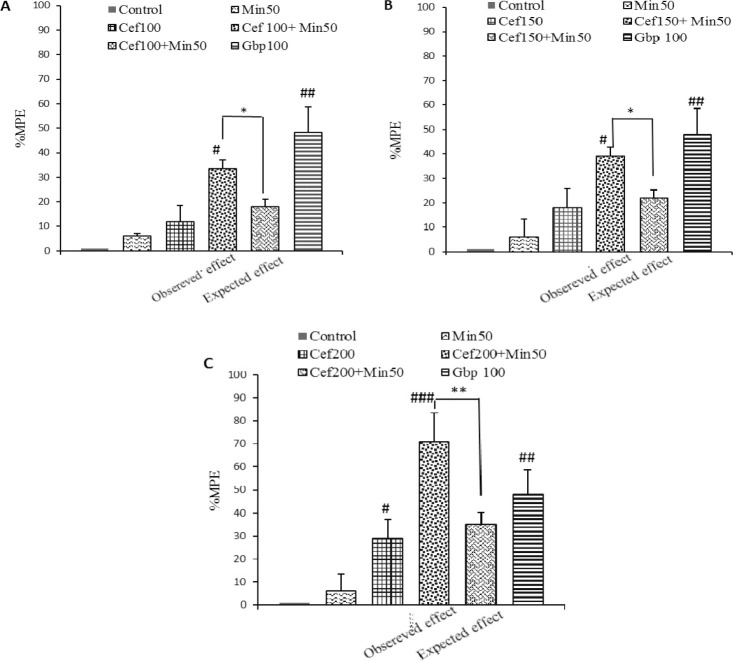
Glutamate neurotoxicity and pro-inflammatory cytokines have an important role in the central sensitization of neuropathic pain. The purpose of the present study was to evaluate anti-hyperalgesic effect of repeated administration of ceftriaxone, which selectively activates and increases the expression of glutamate transporter, as well as minocycline, a selective inhibitor of microglia activation, either alone or together in Wistar rats subjected to the chronic constriction injury (CCI) of sciatic nerve. Ceftriaxone (100, 150 and 200 mg/kg) and minocycline (25, 50 and 100 mg/kg) were administered intraperitoneally from the day of surgery for seven consecutive days. Thermal hyperalgesia was assessed by focal radiant heat source on the hind paw of animals one day before surgery and on 3, 5, 7, 10 and 14 days following that. Ceftriaxone dose dependently, attenuated thermal hyperalgesia in animals. None of the administered doses of minocycline affected the CCI induced-thermal hyperalgesia in neuropathic animals. A fixed dose of minocycline (50 mg/kg) combined with three different doses of ceftriaxone administered for 7 consecutive days yielded a potentiating effect in the enhancing latency time to noxious thermal stimulus remaining until the 14th day post-surgery. The results suggest that modulation of microglia activity could have a supportive role in the improvement of CCI-induced thermal hyperalgesia and combination of such classes of drugs which have no antibiotic effects could be a new and promising therapeutic strategy for treatment.
Keywords: Ceftriaxone; Minocycline; Neuropathic pain; Rat; Thermal hyperalgesia.
Figures
References
-
- Kingery WS. A critical review of controlled clinical trials for peripheral neuropathic pain and complex regional pain syndromes. Pain. 1997;73:123–139. - PubMed
-
- Woolf CJ, Mannion RJ. Neuropathic pain: Etiology, symptoms, mechanisms, and management. Lancet. 1999;353:1959–1964. - PubMed
-
- Sah DWY, Ossipo MH, Porreca F. Neurotrophic factors as novel therapeutics for neuropathic pain. Nat Rev Drug Discov. 2003;2:460–472. - PubMed
-
- Vranken JH. Mechanisms and treatment of neuropathic pain. Cent Nerv Syst Agents Med Chem. 2009;9:71–78. - PubMed
-
- Wagner R, Myers RR. Schwann cells produce tumor necrosis factor alpha: expression in injured and non-injured nerves. Neuroscience. 1996;73:625–629. - PubMed
LinkOut - more resources
Full Text Sources